BACKGROUND
The heart is a pump responsible for maintaining blood supply to the body. It has four chambers. The two upper chambers (the right atrium and left atrium) are the chambers that receive blood as it returns from the body via the veins. The lower chambers (the right and left ventricle) are the chambers responsible for pumping the blood out to the body via the arteries. Like any pump, the heart has an electrical system that controls how it functions.
Normal heart rhythm.
In order for the heart to do its work (pumping blood throughout the body), it needs a sort of spark plug or electrical impulse to generate a heartbeat. Normally this electrical impulse begins in the upper right chamber of the heart (in the right atrium) in a place called the sino-atrial (SA) node. The SA node is the natural pacemaker of the heart. The SA node gives off electrical impulses to generate a heartbeat in the range of 60 to 100 times per minute. If you are exercising, doing strenuous work or are under stress, your heart rate will be faster. When you rest or sleep your heart rate will slow down. If you take certain medications, your heart rate may be slower.
From the Sinus Node, the electrical impulse is relayed along the heart’s conduction system. It spreads throughout both the right and left atria causing them to contract evenly.
When the impulse spreads over the right atrium it reaches the atrio-ventricular (AV) node. This is a very important structure in the heart because it is the only electrical connection between the top chambers and the bottom chambers. It is therefore the only way in which an electrical impulse can reach the pumping chambers (the ventricles). The impulse spreads through the AV node and down into the lower chambers or ventricles of the heart. This causes them to contract and pump blood to the lungs and body.
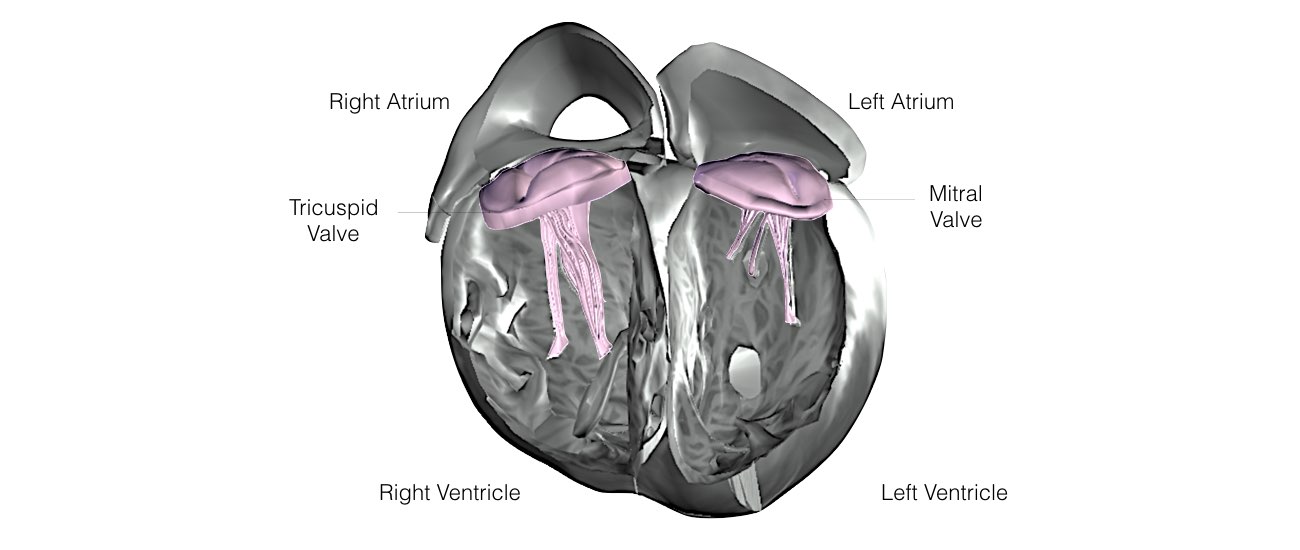
The heart is made up of four chambers. The top two chambers are call the Atria and the bottom two chambers are called the Ventricles.
The top and bottom chambers are separated by two valves the Tricuspid Valve and the Mitral Valve.
The Tricuspid Valve separates the Right Atrium from the Right Ventricle
The Mitral Valve separates the Left Atrium from the Left Ventricle
Slide 1 of 8
The top and bottom chambers are separated by two valves the Tricuspid Valve and the Mitral Valve.
The Tricuspid Valve separates the Right Atrium from the Right Ventricle
The Mitral Valve separates the Left Atrium from the Left Ventricle
Slide 1 of 8
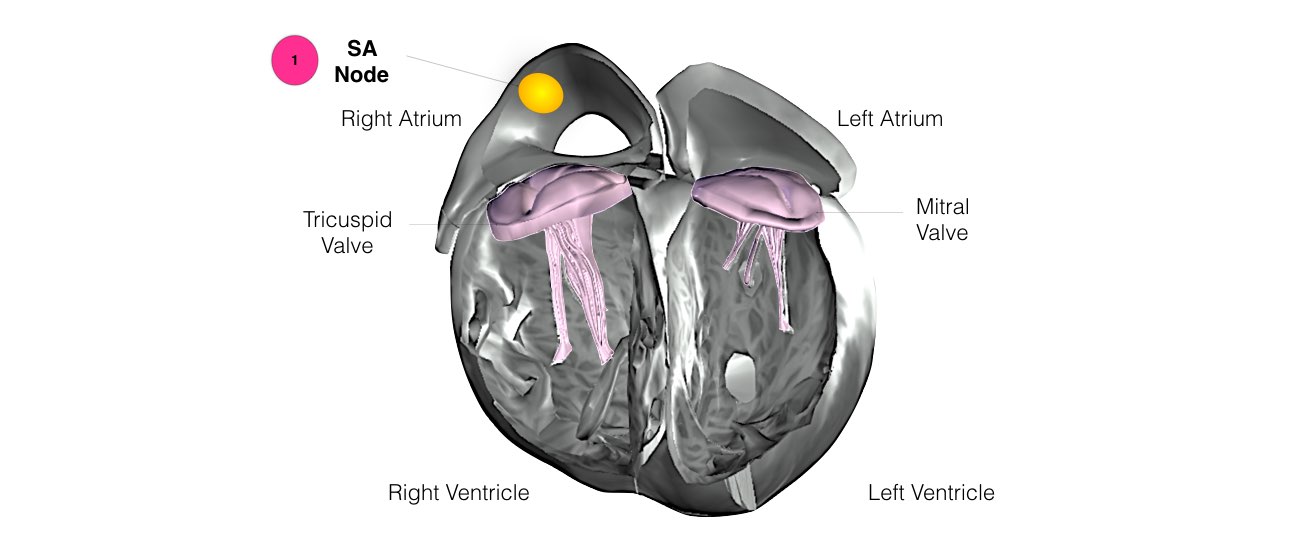
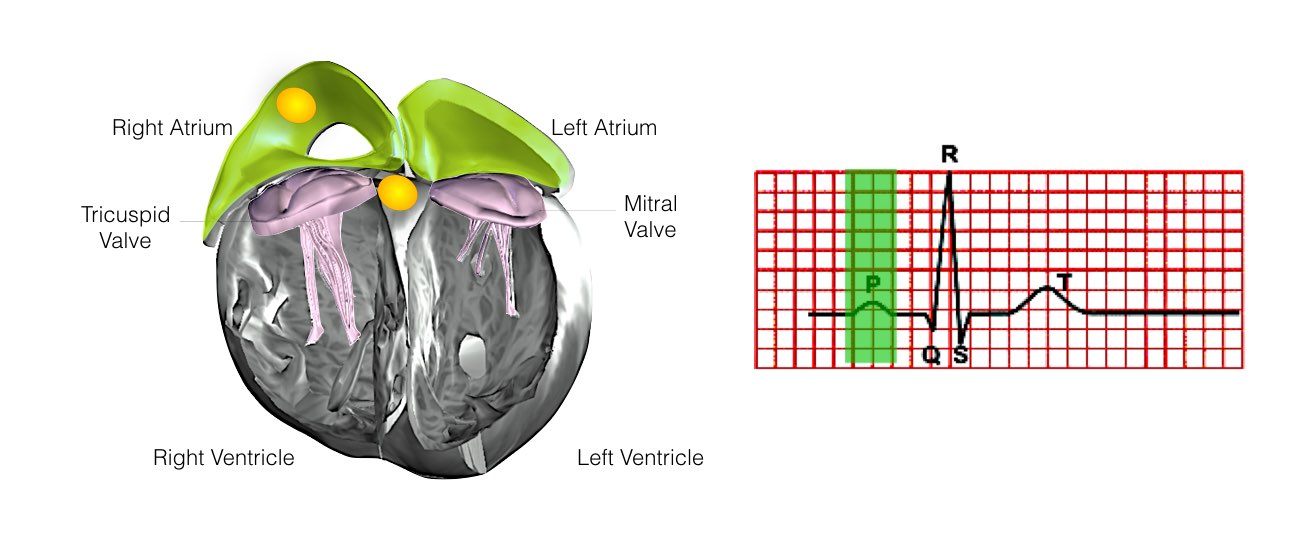
1) The normal heart beats starts in the Sino-Atrial Node located in the Right Atrium. This acts as the spark plug to start the heart.
Slide 2 of 8
Slide 2 of 8
The normal heart beats starts in the Sino-Atrial Node located in the Right Atrium. This acts as the spark plug to start the heart.
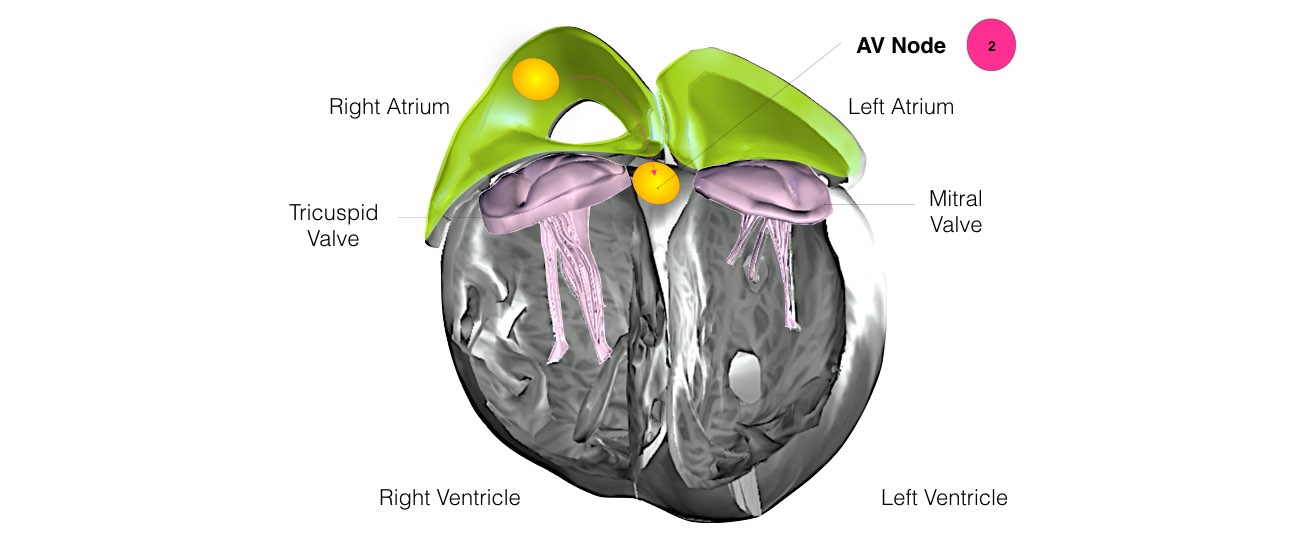
2) Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
Slide 3 of 8
2) Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
Slide 3 of 8
The normal heart beats starts in the Sinus Node located in the Right Atrium. This acts as the spark plug to start the heart.
Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
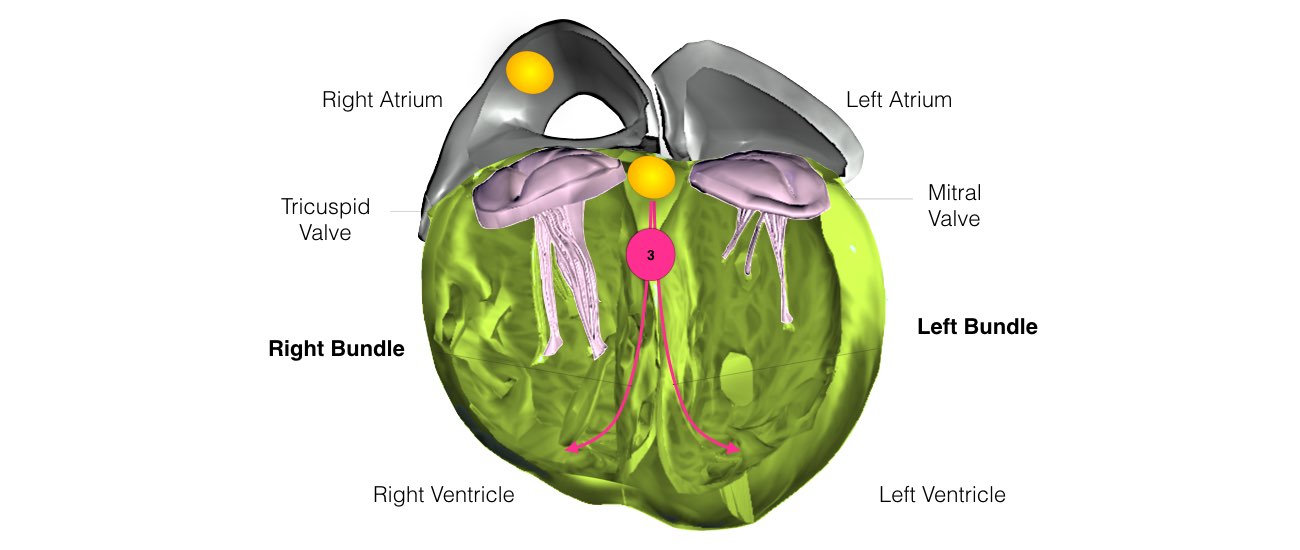
3) After electrical conduction passes through the AV node it travels down the Left and Right Bundle Branches which activates the Ventricles and tells them to contract.
Slide 4 of 8
Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
3) After electrical conduction passes through the AV node it travels down the Left and Right Bundle Branches which activates the Ventricles and tells them to contract.
Slide 4 of 8
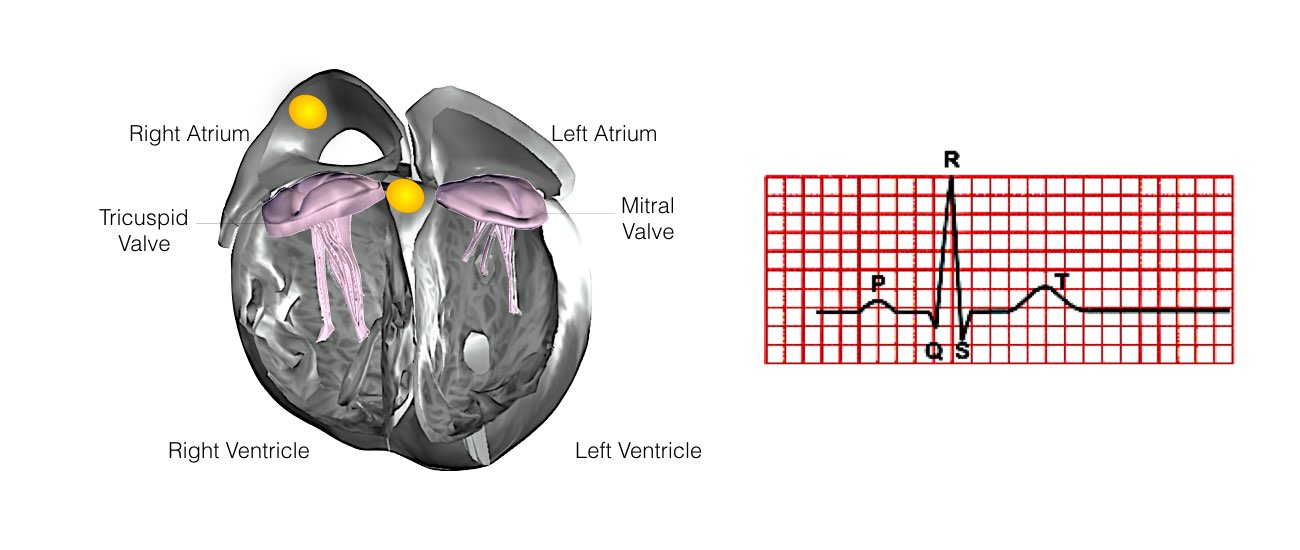
The heart's normal contraction can be seen on the ECG. This ECG shows normal sinus rhythm and is made up of a series of waves called the P, QRS and T wave.
Slide 5 of 8
Slide 5 of 8
Atrial activation is represented by the ‘P-Wave’ on the ECG.
Slide 6 of 8
Slide 6 of 8
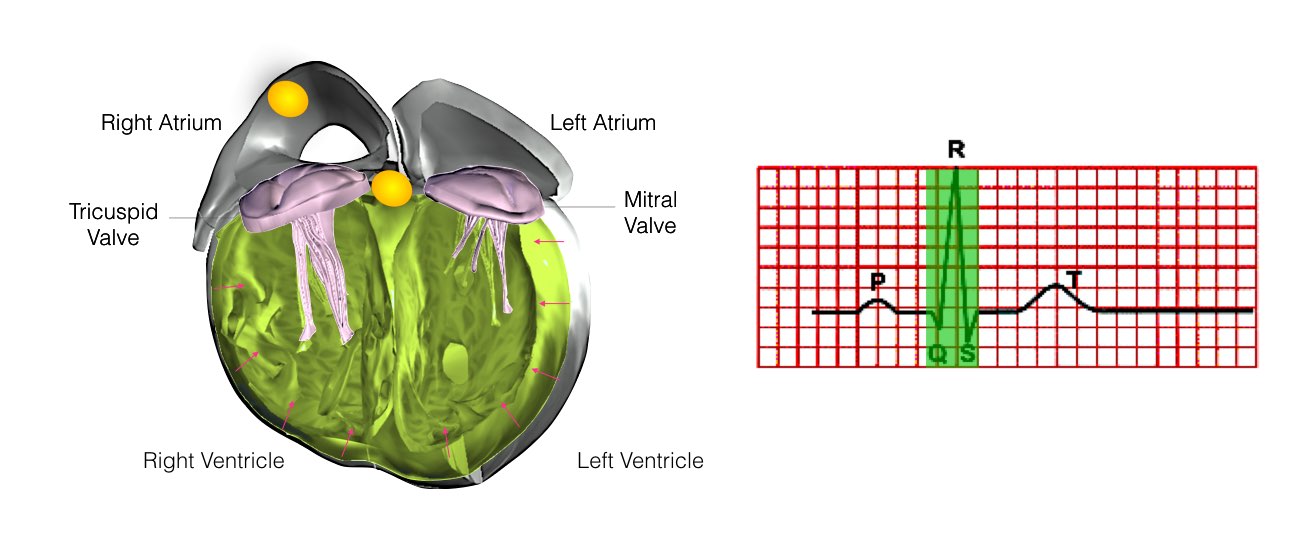
Ventricular activation is represented by the ‘QRS’ complex on the ECG. This normally takes less than 120 milliseconds.
During this time the Ventricles contract and blood is pumped from the heart to the lungs and through the aorta to the rest of the body.
Slide 7 of 8
During this time the Ventricles contract and blood is pumped from the heart to the lungs and through the aorta to the rest of the body.
Slide 7 of 8
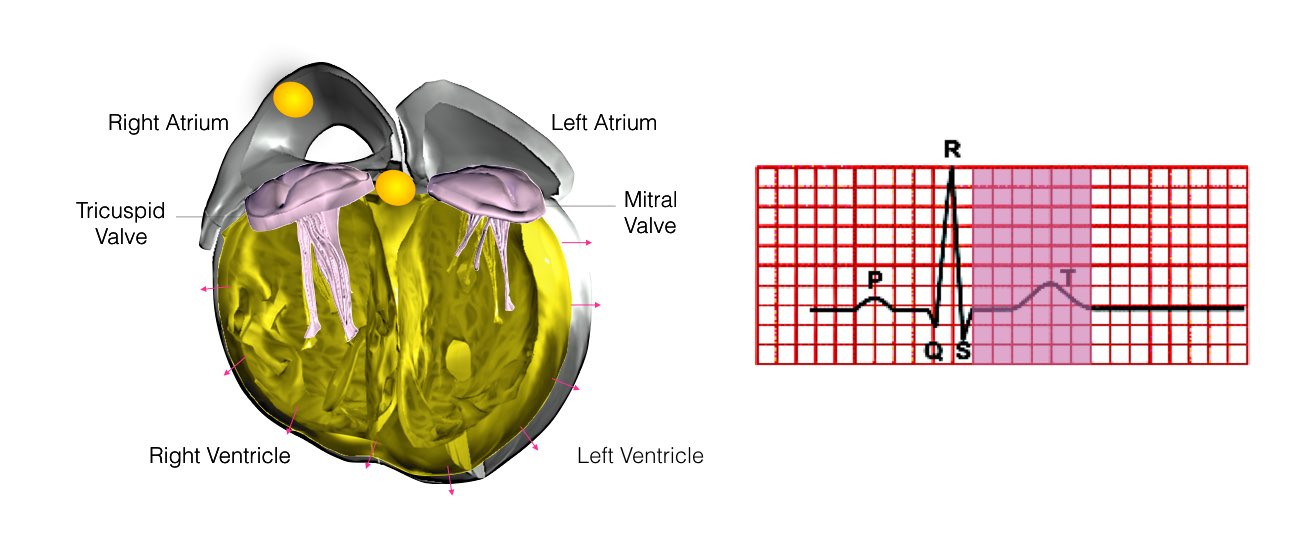
The final wave is called the T wave. During this phase the Ventricles relax. This normally takes less than 450 milliseconds.
Slide 8 of 8
Slide 8 of 8
What is Supraventricular tachycardia?
In some hearts, an abnormal heart rhythm develops in the top part of the heart when an electrical impulse either starts from a different location other than the SA node, or follows a route (or pathway) that is not normally present. When this occurs the heart will suddenly start racing. The heart rate is usually over 150 beats per minute and often over 200 beats per minute. Certain things in some people can trigger episodes. These include caffeine, alcohol, anxiety, exercise or sudden movements such as bending over. However, often these episodes can occur at any time without a trigger. During an episode, you will usually be aware of the rapid beating of your heart.
Other symptoms might include dizziness (blacking out may occur but is unusual), shortness of breath, sweating, chest pain and anxiety. After an episode it is usual to feel very tired.
Is Supraventricular tachycardia dangerous?
In the vast majority of cases SVT is a benign condition. This means that it will not cause sudden death, will not damage the heart or cause a heart attack and will not shorten life expectancy. There are some rare exceptions that will be discussed with you if relevant.
How does Supraventricular tachycardia occur ?
There are 3 main types of SVT. It will not always be obvious which type of SVT you have prior to the electrical study of your heart.
1. AV Nodal Re-entry Tachycardia (AVNRT)
This is the most common form of SVT. An abnormal short circuit (circular conduction) occurs near the AV node. Instead of a single AV node between the top and bottom chambers, there is a second connection that is abnormal. This extra connection has been present since birth. As a result of having 2 connections a short-circuit can occur.
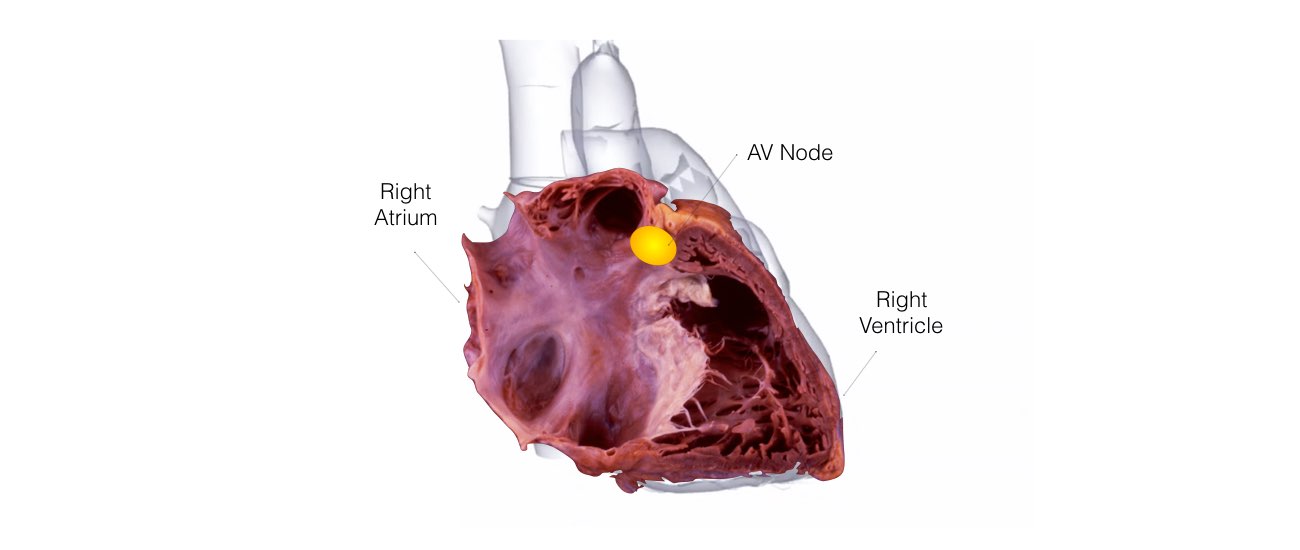
AV Node Re-entrant Tachycardia is the most common form of SVT.
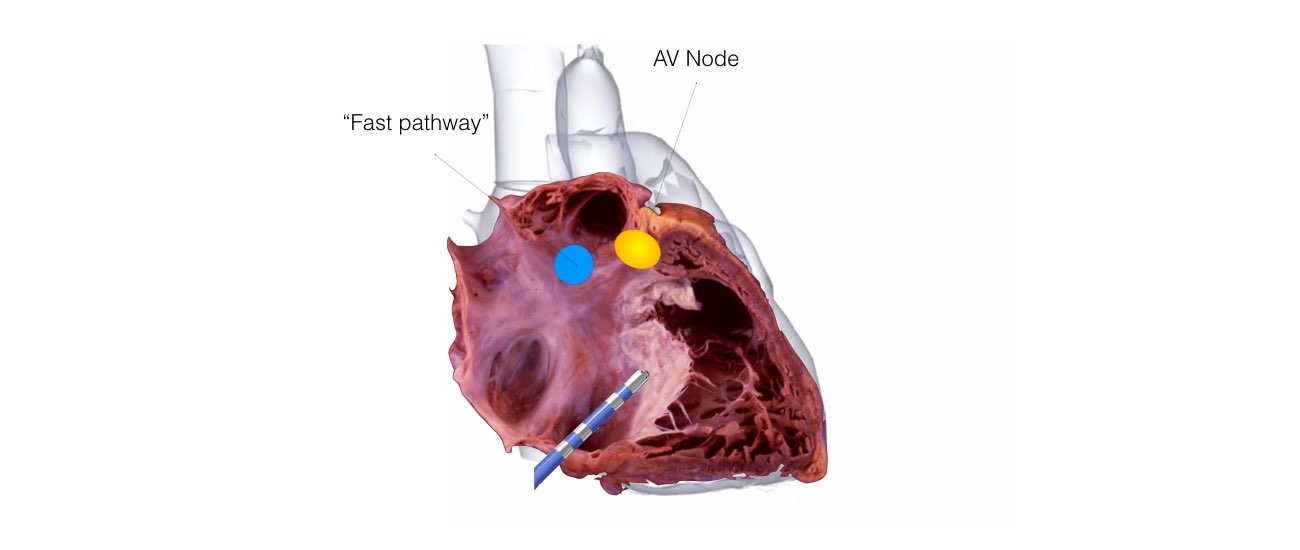
It is a caused by a small ‘short-circuit’ on the right side of the heart in the right atria.
Slide 1 of 6
It is a caused by a small ‘short-circuit’ on the right side of the heart in the right atria.
Slide 1 of 6
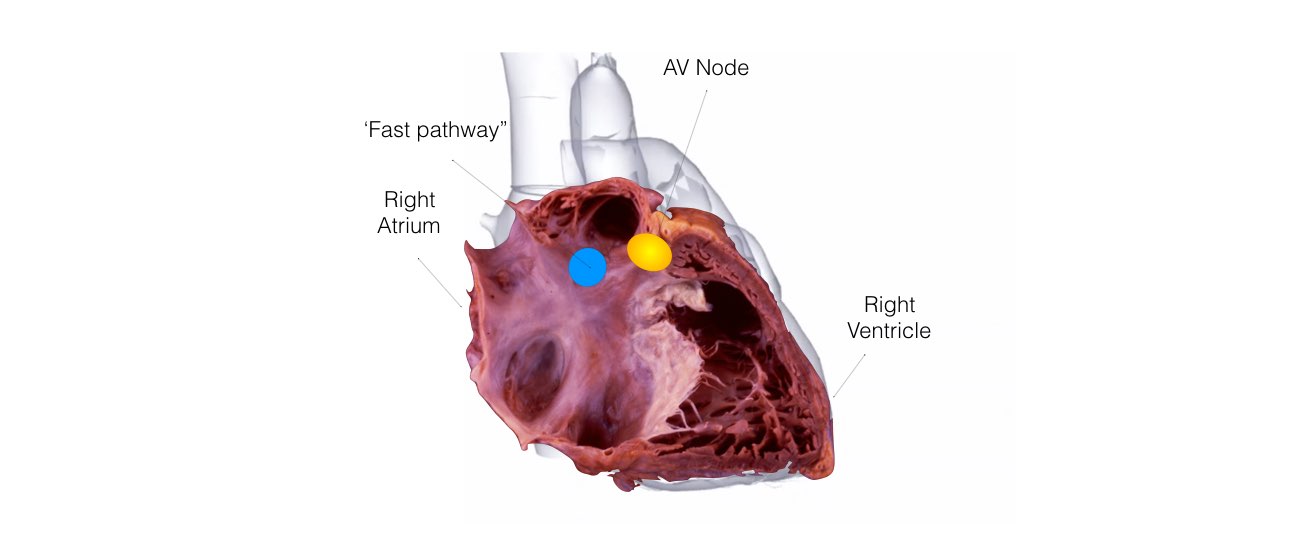
Most patients only have a single wire that inputs to the AV node called the ‘Fast-Pathway’.
Slide 2 of 6
Slide 2 of 6
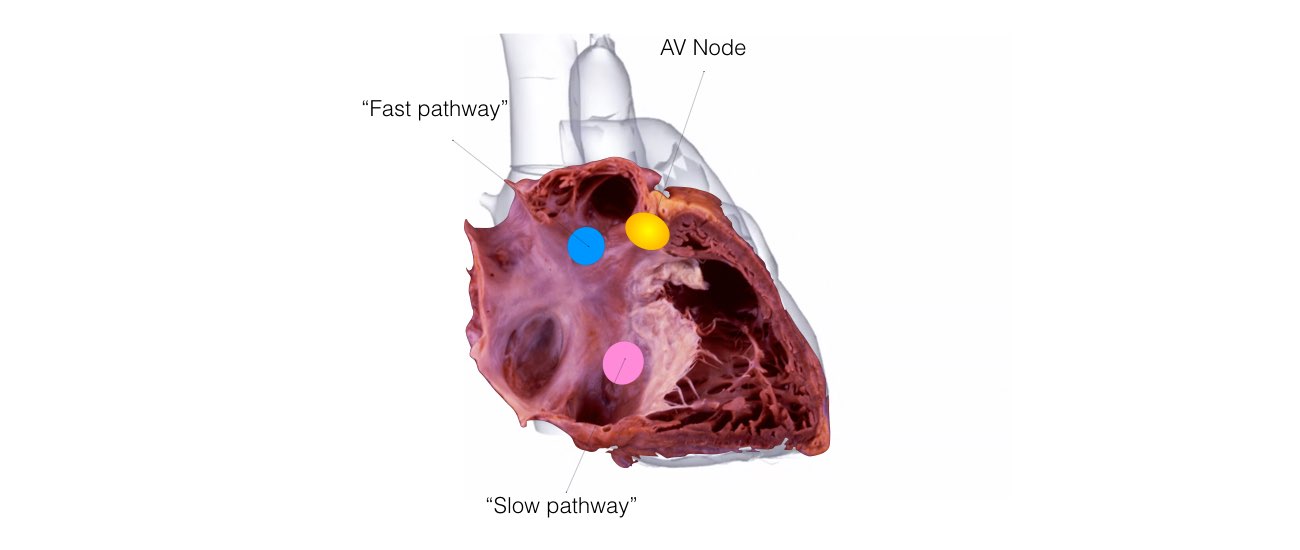
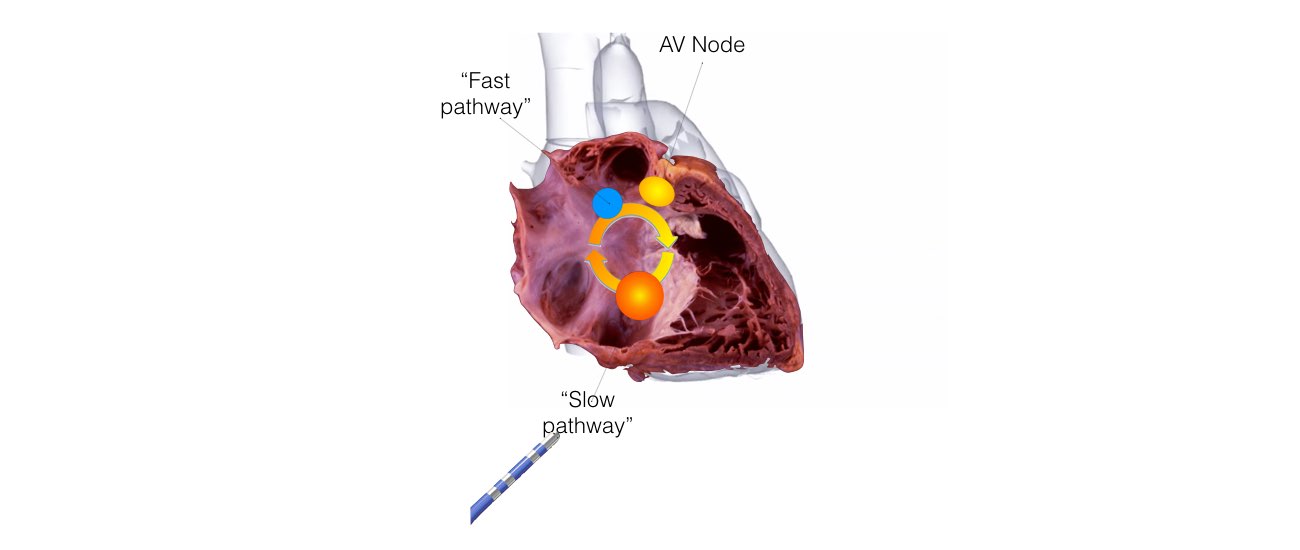
Patients with AVNRT are born with two wires connecting the atrium and the ventricles. They have an extra wire called the “Slow Pathway".
Slide 3 of 6
Slide 3 of 6
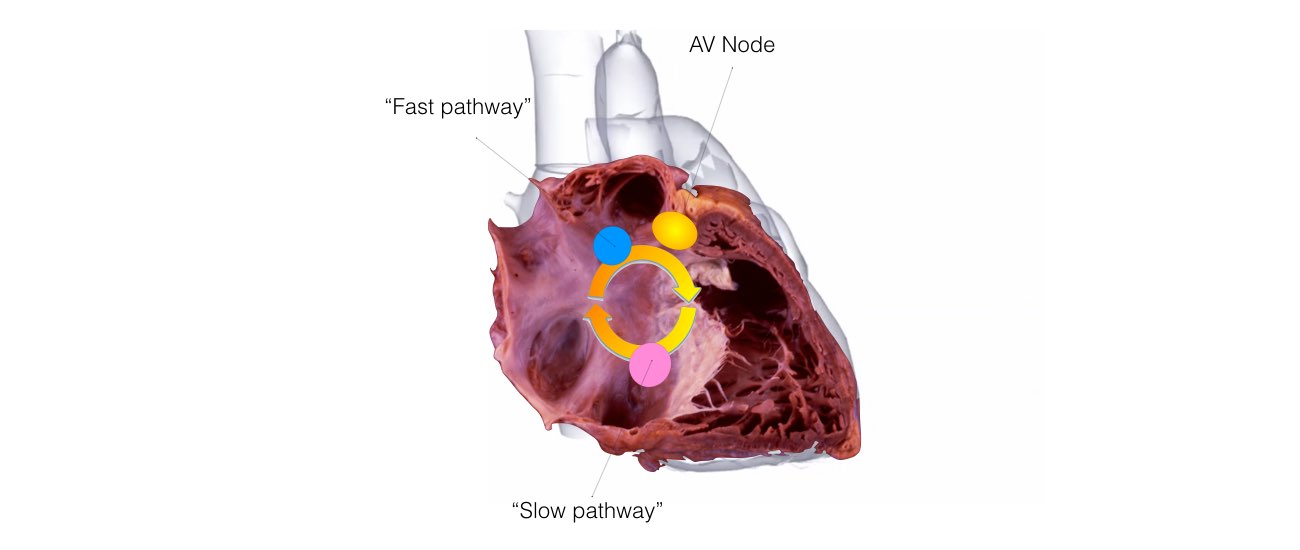
In patients with AVNRT these two wires form a ‘short-circuit’ that leads to symptomatic racing of the heart or palpitations.
This ‘short-circuit’ can be treated with a simple procedure called radio-frequency ablation.
Slide 4 of 6
This ‘short-circuit’ can be treated with a simple procedure called radio-frequency ablation.
Slide 4 of 6
During this procedure a small catheter is passed up from the leg to the heart. It is then positioned at the
Slow Pathway region in the right atrium.
2-3 minutes of radio-frequency energy is then delivered to the this area cauterising the slow pathway. Because the slow-pathway is cauterised, the AVNRT circuit cannot re-form.
Slide 5 of 6
2-3 minutes of radio-frequency energy is then delivered to the this area cauterising the slow pathway. Because the slow-pathway is cauterised, the AVNRT circuit cannot re-form.
Slide 5 of 6
Ablation of AVNRT is successful in 90-95% of patients.
Slide 6 of 6
Slide 6 of 6
2. Re-entrant Tachycardia and Wolff Parkinson White Syndrome
Abnormal circular conduction utilising the AV node and an “accessory pathway” connecting the atria and ventricles. This extra connection has been present since birth. As a result of having 2 connections a short-circuit can occur. This condition is sometimes termed the Wolff-Parkinson-White Syndrome or WPW.
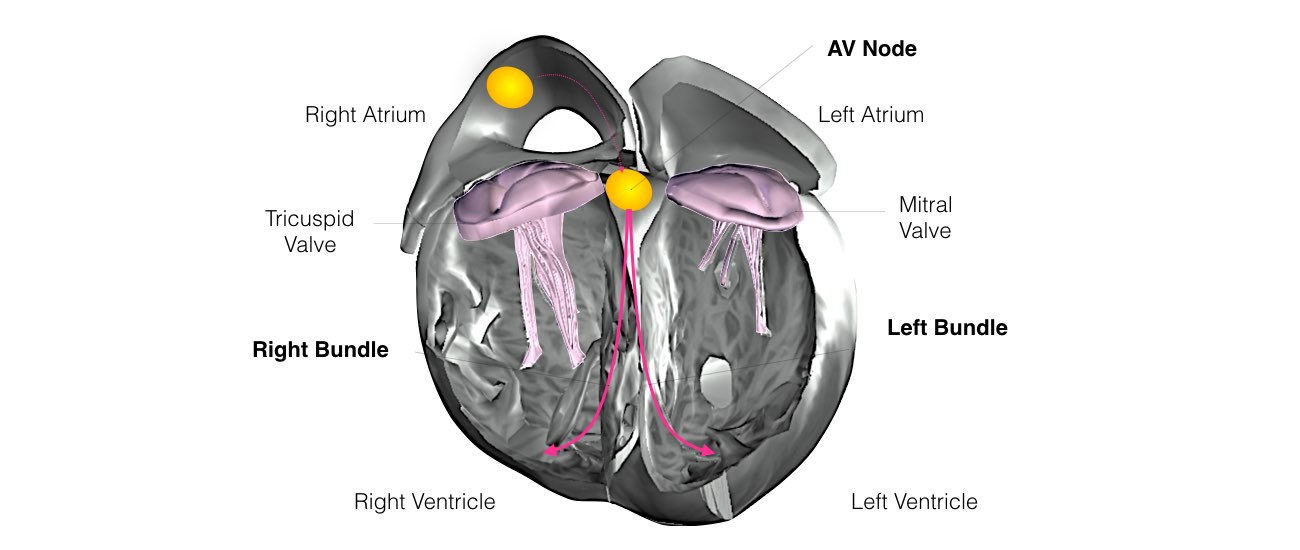
Normally the AV Node acts as the ‘gate-keeper’ and all electrical signals from atria must pass through the AV Node before travelling down the Left and Right Bundle Branches to activate the Ventricles.
Slide 1 of 7
Slide 1 of 7
Normally the AV Node acts as the ‘gate-keeper’ and all electrical signals from atria must pass through the AV Node before travelling down the Left and Right Bundle Branches to activate the Ventricles.
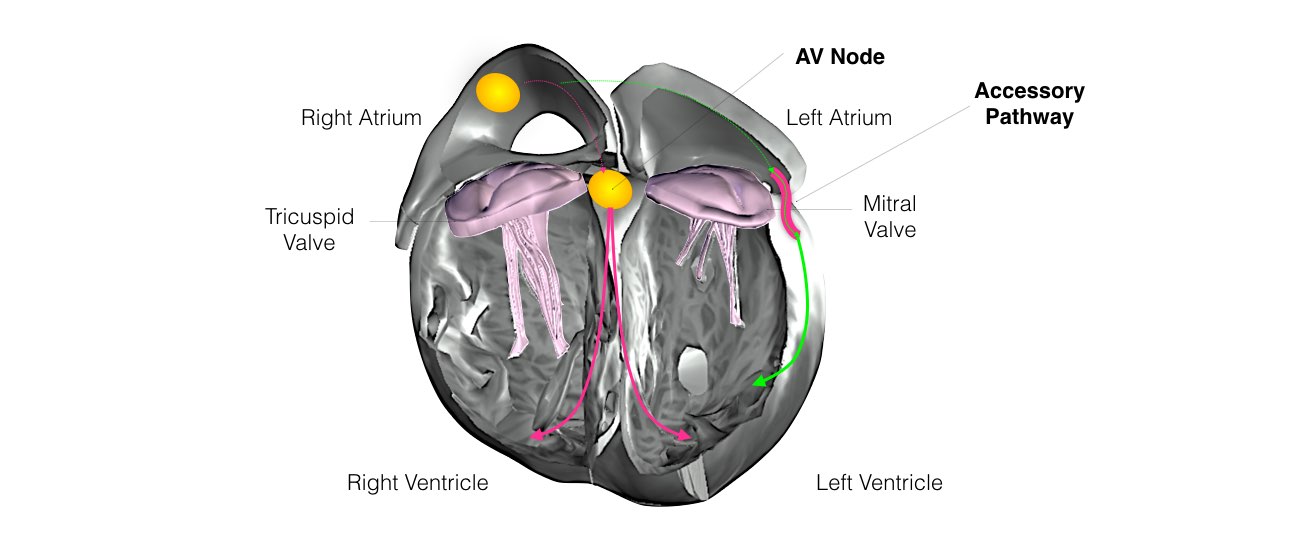
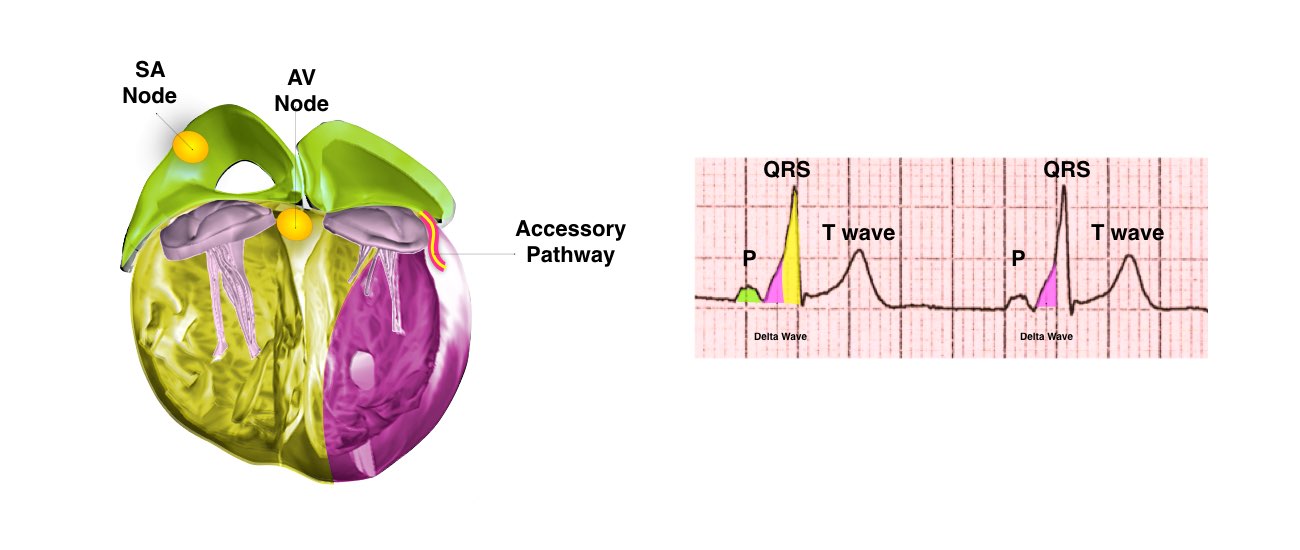
Some patients are born with an extra electrical fibre that connects the atria and the ventricles. These are called Accessory Pathways and provide an extra electrical connection from the Atria to the Ventricles bypassing the AV Node.
Slide 2 of 7
Some patients are born with an extra electrical fibre that connects the atria and the ventricles. These are called Accessory Pathways and provide an extra electrical connection from the Atria to the Ventricles bypassing the AV Node.
Slide 2 of 7
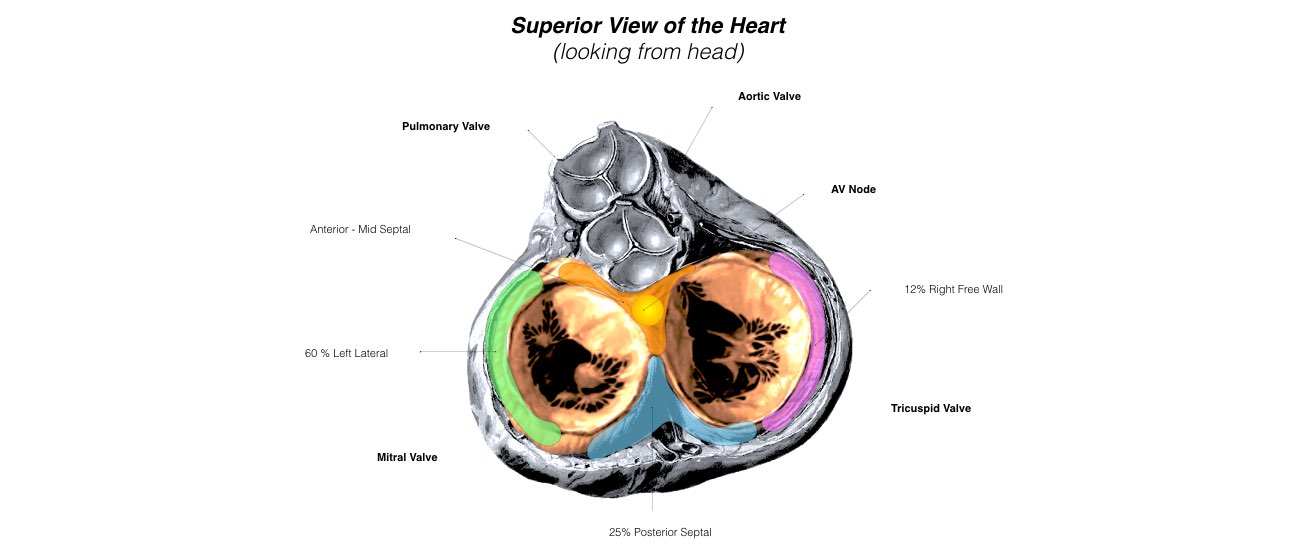
Accessory pathways are commonly found in certain locations around the Mitral and Tricuspid Valves.
The three most common location is in a Left Lateral location (60%) around the mitral valve, then in a Posterior-Septal location between the valves (25%) and finally around the free wall of the Tricuspid Valve.
The accessory pathways located the vicinity of the AV node (anterior/ mid septal locations) are hardest to treat with catheter ablation as they can be quite close to the normal AV Node.
Slide 3 of 7
The three most common location is in a Left Lateral location (60%) around the mitral valve, then in a Posterior-Septal location between the valves (25%) and finally around the free wall of the Tricuspid Valve.
The accessory pathways located the vicinity of the AV node (anterior/ mid septal locations) are hardest to treat with catheter ablation as they can be quite close to the normal AV Node.
Slide 3 of 7
In WPW, the accessory pathway acts as a bypass tract connecting the atria to the ventricles,
‘short-circuiting’ the AV node.
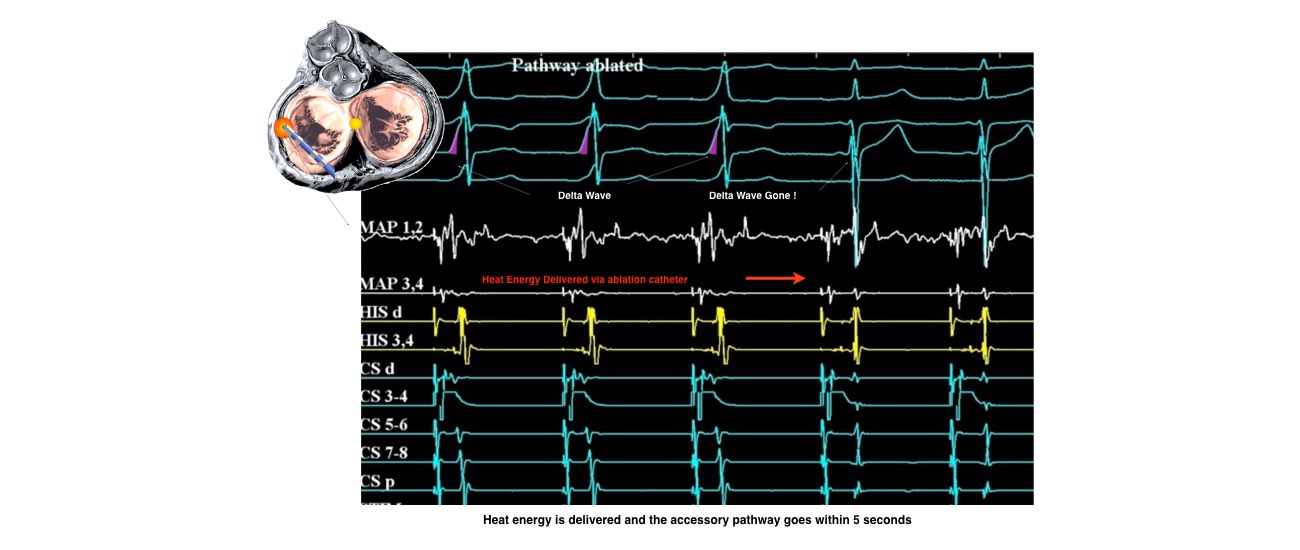
This leads to much earlier activation of the ventricles compared to normal (called pre-excitation). This is results in the classical ‘delta-wave’ on the ECG (purple). The rest of the ventricle is activated via the slower conducting AV node.
Slide 4 of 7
This leads to much earlier activation of the ventricles compared to normal (called pre-excitation). This is results in the classical ‘delta-wave’ on the ECG (purple). The rest of the ventricle is activated via the slower conducting AV node.
Slide 4 of 7
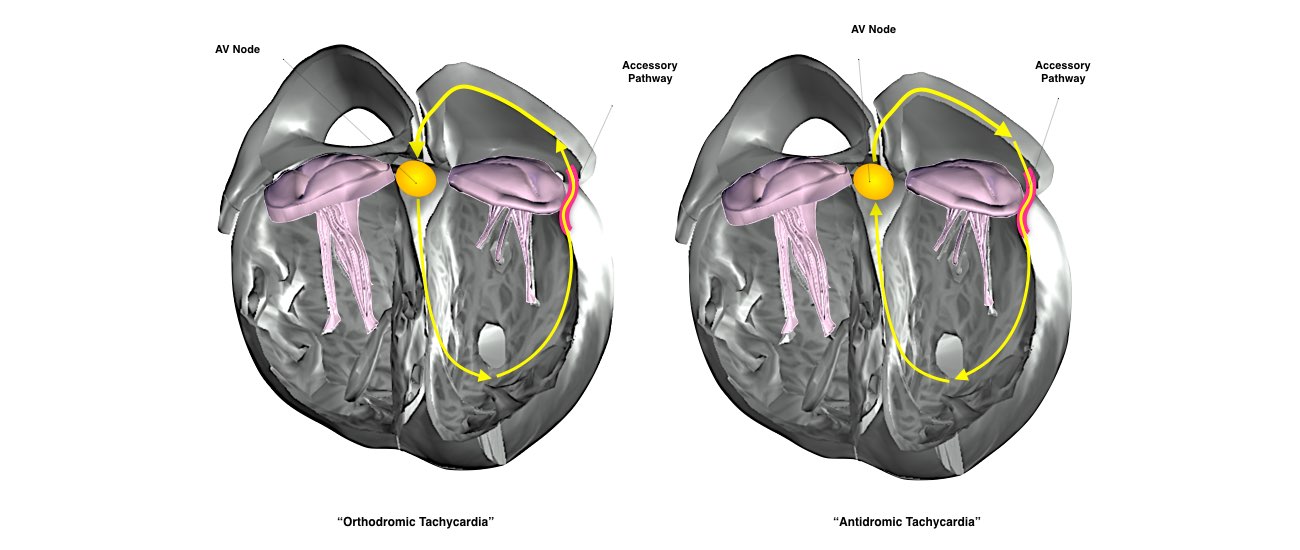
Accessory pathways provide the ‘short-circuit’ required for re-entry circuits and can result in palpitations.
The two circuits that can occur are shown. The most common circuit utilises the accessory pathway to conduct from the Ventricle back to the Atrium. This is called “Orthodromic tachycardia” and leads to a narrow complex SVT on the 12 lead ECG.
The other circuit uses the accessory pathway to conduct from the Atria to the Ventricles. This is called “Antidromic Tachycardia” and results in a wide complex SVT on the 12 lead ECG
“Both circuits use the AV node as one limb to complete the re-entry circuit.
Slide 5 of 7
The two circuits that can occur are shown. The most common circuit utilises the accessory pathway to conduct from the Ventricle back to the Atrium. This is called “Orthodromic tachycardia” and leads to a narrow complex SVT on the 12 lead ECG.
The other circuit uses the accessory pathway to conduct from the Atria to the Ventricles. This is called “Antidromic Tachycardia” and results in a wide complex SVT on the 12 lead ECG
“Both circuits use the AV node as one limb to complete the re-entry circuit.
Slide 5 of 7
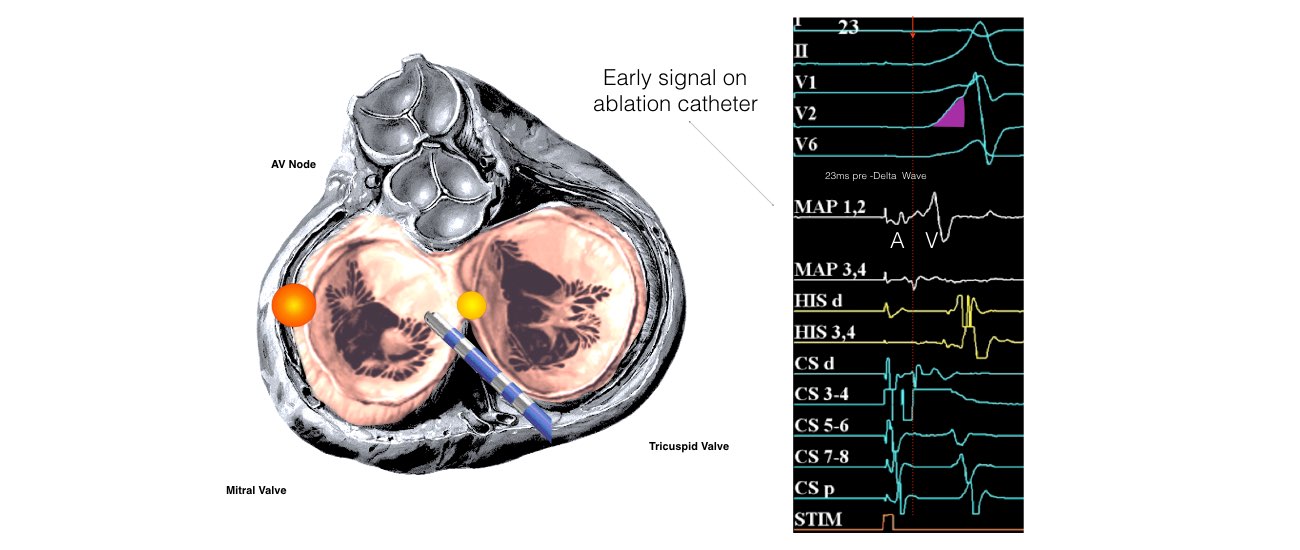
Catheter ablation involves mapping around the Mitral or Tricuspid valve to find the earliest signal from the accessory pathway.
One to two minutes of heat energy is delivered via the ablation catheter and accessory pathway is destroyed.
Slide 6 of 7
One to two minutes of heat energy is delivered via the ablation catheter and accessory pathway is destroyed.
Slide 6 of 7
We know if we are successful immediately as the accessory pathway usually disappears within 5 seconds of heat energy. Success rates for accessory pathway ablation procedure is over 95%
Slide 7 of 7
Slide 7 of 7
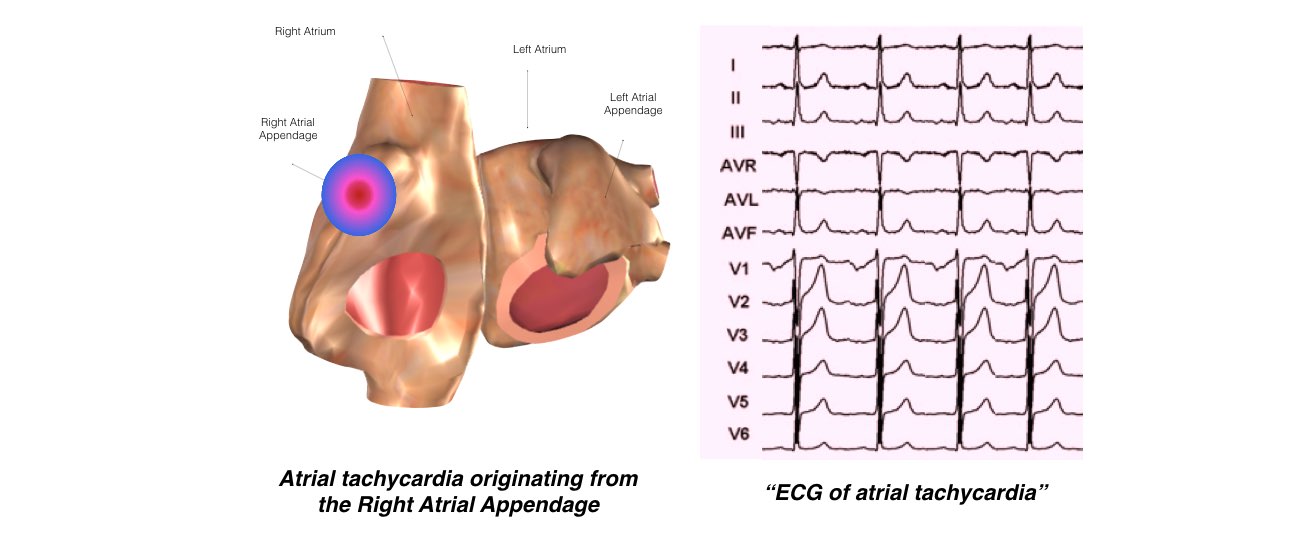
Atrial Tachycardia
This is the least common form of SVT. There is an extra abnormal origin of the electrical impulse from a small area in the atria other than the SA node. It is not known when or why such an extra focus develops

The top chambers of the heart are called atria. They sit at the back of the heart.
Slide 1 of 5
Slide 1 of 5
Atrial tachycardias are caused by small nests of rapidly firing cells within normal atrial tissue. They are called focal tachycardias.
Rapid firing of these abnormal cells leads to a rapid heart rate which can cause symptoms such as palpitations and shortness of breath.
Slide 2 of 5
Rapid firing of these abnormal cells leads to a rapid heart rate which can cause symptoms such as palpitations and shortness of breath.
Slide 2 of 5
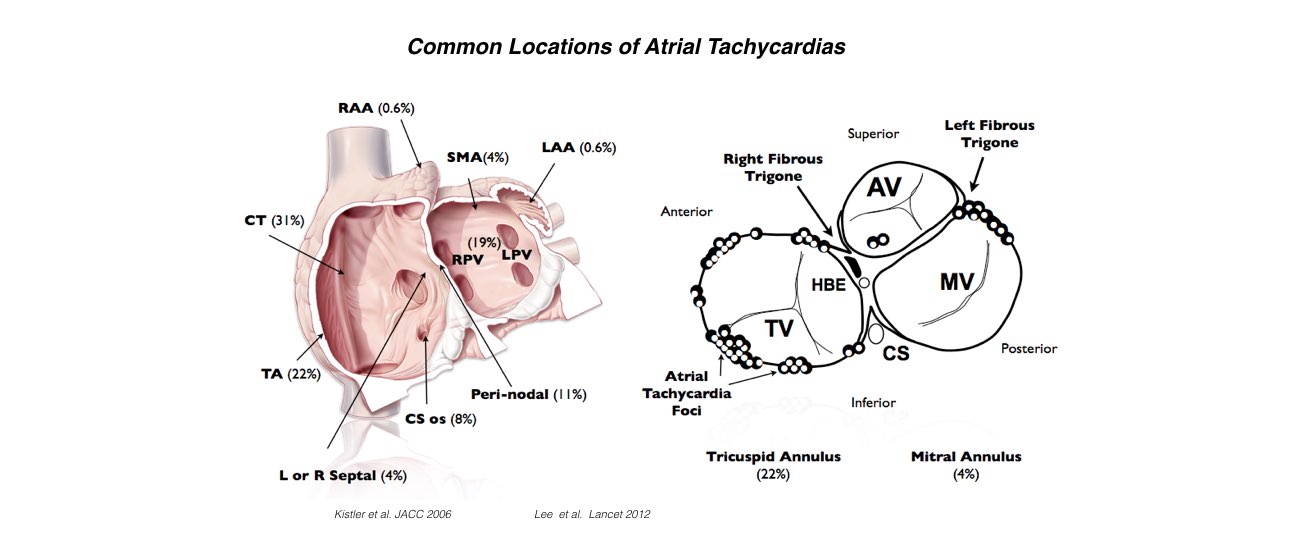
Our research has shown that atrial tachycardias do not occur in random locations. They seem to occur in common locations within the right atrium and left atrium and around the tricuspid and mitral valves.
Slide 3 of 5
Slide 3 of 5
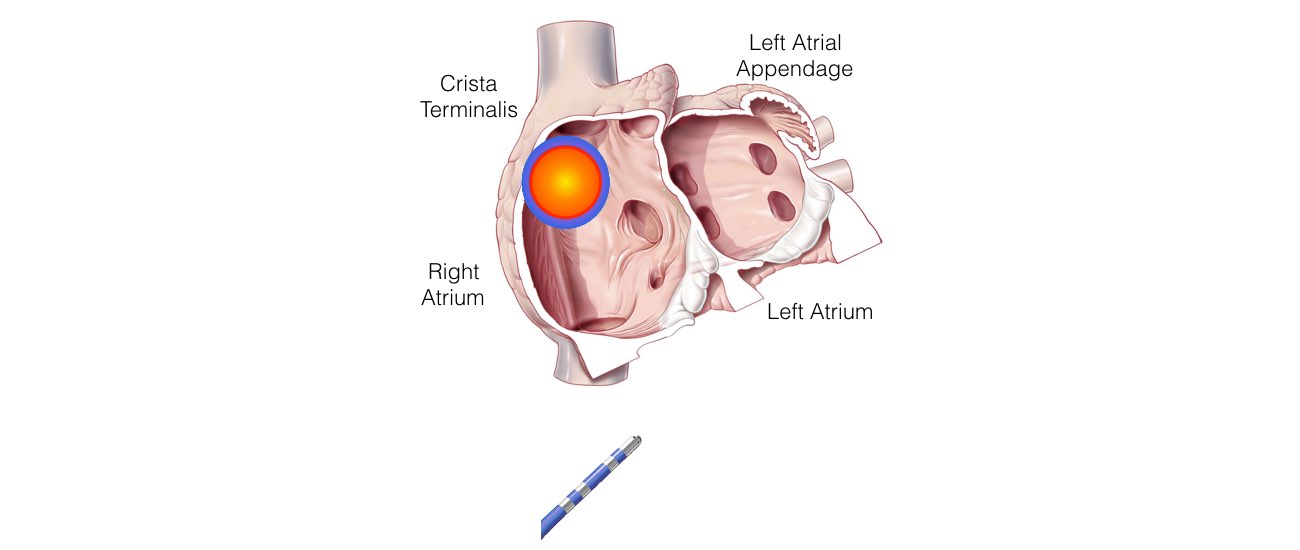
Atrial Tachycardias can be treated with an ablation procedure. We need the focus to be firing off on the day for the procedure to be successful.
A catheter is advanced from the leg to the atria. The catheter is used to map the atria to find the earliest site of activity.
Because the rapid focus radiates out like dropping a pebble in a pond, it is a matter of find the site of earliest firing. Heat energy is then delivered to cauterise the small areas of rogue cells.
Slide 4 of 5
A catheter is advanced from the leg to the atria. The catheter is used to map the atria to find the earliest site of activity.
Because the rapid focus radiates out like dropping a pebble in a pond, it is a matter of find the site of earliest firing. Heat energy is then delivered to cauterise the small areas of rogue cells.
Slide 4 of 5
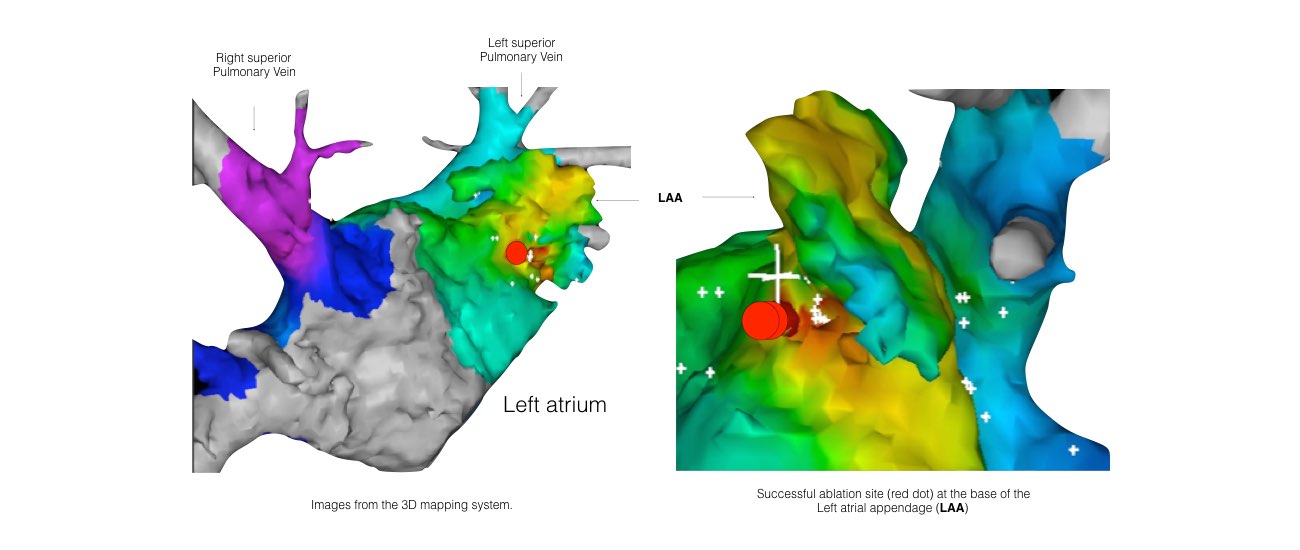
A 3D computer mapping system is used to guide the ablation procedure. It allows us to see the catheter and the heart in 3D so we know exactly where we are.
This means we can be extremely accurate in finding the focus and it also reduces the amount of radiation exposure to the patient and the staff.
Slide 5 of 5
This means we can be extremely accurate in finding the focus and it also reduces the amount of radiation exposure to the patient and the staff.
Slide 5 of 5

