AF Ablation
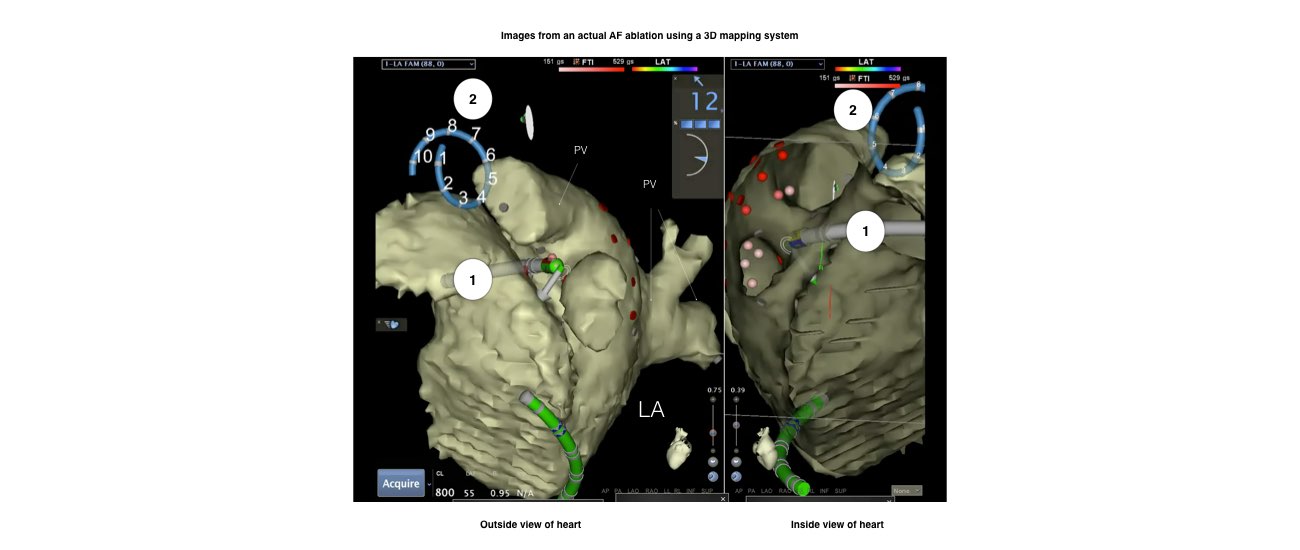
Atrial fibrillation is due to abnormal signals in the pulmonary veins
Atrial fibrillation is due to abnormal signals in the pulmonary veins
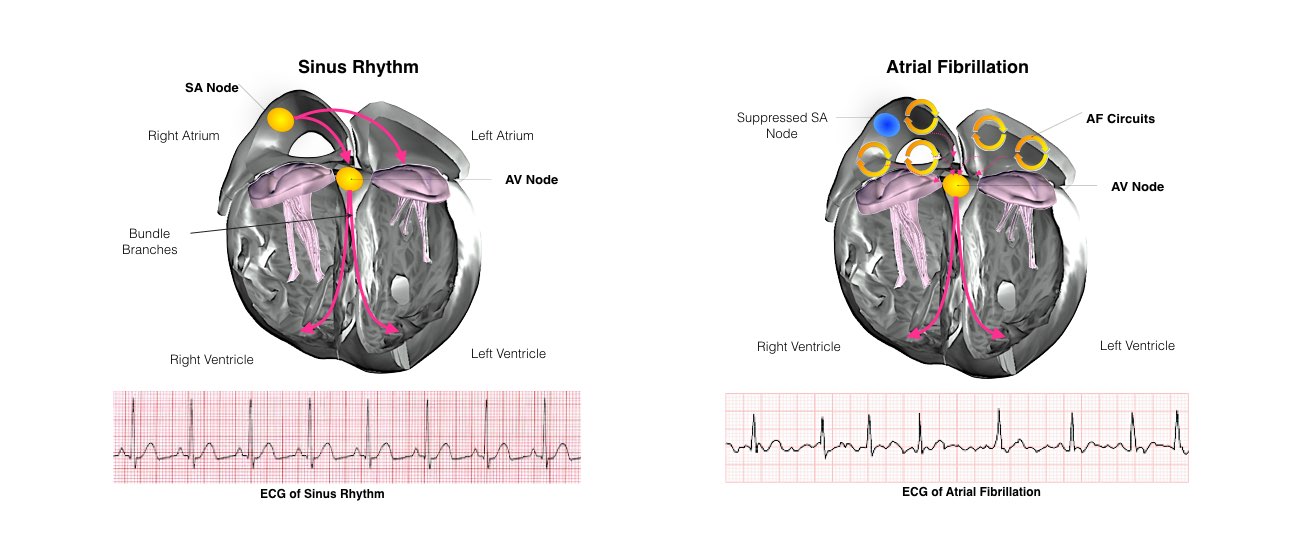
The heart is a pump responsible for maintaining blood supply to the body. It has four chambers. The two upper chambers (the right atrium and left atrium) are the chambers that receive blood as it returns from the body via the veins. The lower chambers (the right and left ventricle) are the chambers responsible for pumping the blood out to the body via the arteries. Like any pump, the heart has an electrical system that controls how it functions.
In order for the heart to do its work (pumping blood throughout the body), it needs a sort of spark plug or electrical impulse to generate a heartbeat. Normally this electrical impulse begins in the upper right chamber of the heart (in the right atrium) in a place called the sino-atrial (SA) node. The SA node is the natural pacemaker of the heart. The SA node gives off electrical impulses to generate a heartbeat in the range of 60 to 100 times per minute. If you are exercising, doing strenuous work or are under stress, your heart rate will be faster. When you rest or sleep your heart rate will slow down. If you take certain medications, your heart rate may be slower.
From the Sinus Node, the electrical impulse is relayed along the heart’s conduction system. It spreads throughout both the right and left atria causing them to contract evenly.
When the impulse spreads over the right atrium it reaches the atrio-ventricular (AV) node. This is a very important structure in the heart because it is the only electrical connection between the top chambers and the bottom chambers. It is therefore the only way in which an electrical impulse can reach the pumping chambers (the ventricles). The impulse spreads through the AV node and down into the lower chambers or ventricles of the heart. This causes them to contract and pump blood to the lungs and body.
Atrial fibrillation is due to the development of electrical short circuits inside the top chambers of the heart. Usually these short circuits begin in the top chamber on the left (left atrium). They are usually triggered by abnormal electrical activity located within the veins that drain blood from the lungs back to the heart (pulmonary veins)
These rapid short circuits have several consequences:
In many people who develop atrial fibrillation the cause is not known. Usually the heart is otherwise sound. In some people atrial fibrillation can develop due to other conditions such as high blood pressure, prior heart attack, weak heart, leaky heart valves, obesity or sleep apnoea. There may be a familial tendency to atrial fibrillation.
Atrial fibrillation can be treated with medication. In some people these medicines can be very effective. In others however, the medications are ineffective and may produce side effects. Your doctor will discuss the different options and the possible side effects of these medications.
Over now more than a decade, a procedure has been developed for cure of atrial fibrillation. This procedure termed RADIOFREQUENCY or CATHETER ABLATION has been available for other types of heart rhythm disturbances for more than 25 years.
Radiofrequency is a type of energy that causes a small burn (ablation) at the tip of the catheter thereby turning the abnormal tissue that was causing the short-circuit into a small scar.
You will be transferred to the Electrophysiology Laboratory (EP lab) from your ward. Usually before leaving the ward your groin will be shaved.
The EP lab has a patient table, X-Ray tube, ECG monitors and other equipment. The staff in the lab will all be dressed in hospital theatre clothes.
Many ECG monitoring electrodes will be attached to your chest area and patches to your chest and back. These patches may momentarily feel cool on your skin.
The anaesthetist will insert an intravenous cannula usually into the back of your hand and a second cannula into the artery. The entire procedure will be performed while you are “asleep” under general anaesthetic.
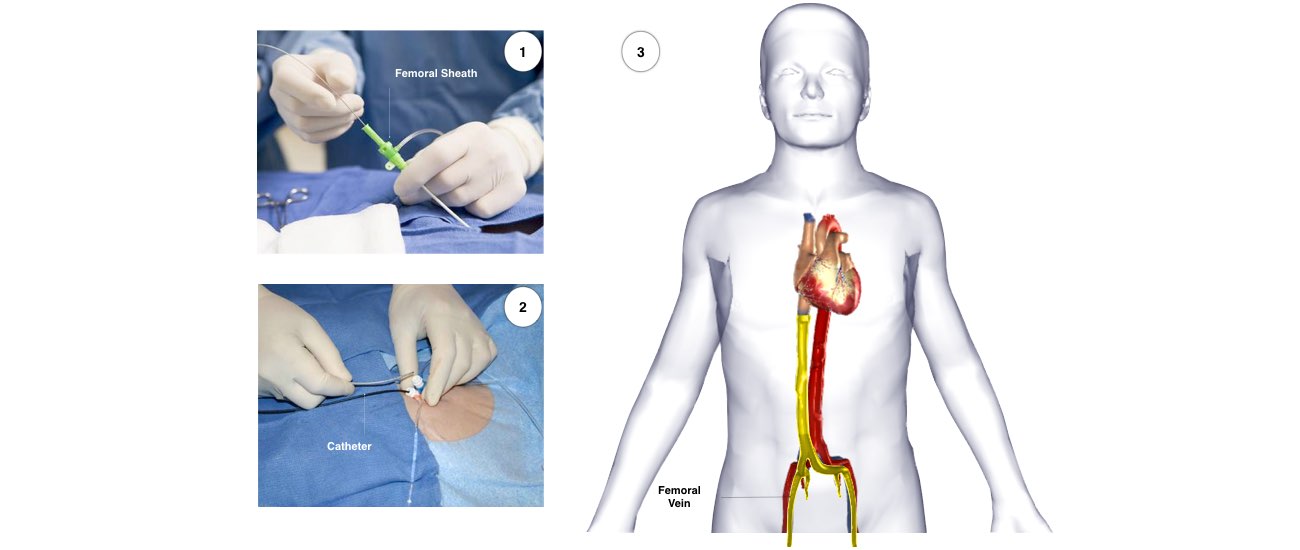
During and after the procedure, blood thinning medication will be administered. During the procedure the heart will be monitored with a special ultrasound probe that is inserted into the oesophagus (swallowing tube). This takes clear pictures of the heart before, during and after the procedure. It will be removed before you wake up. When you are under anaesthetic, special wires (termed electrical catheters) will be inserted into the heart via a vein in the groin area and occasionally also by a vein in the side of the neck. This is routine.
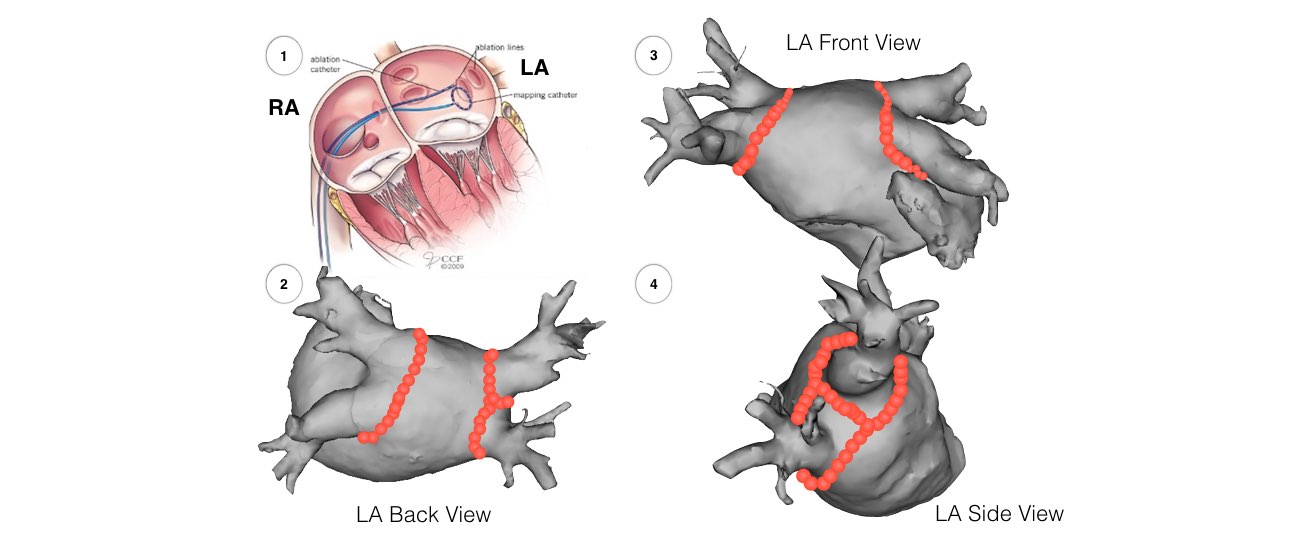
The electrical catheters are positioned using X-Rays, ultrasound and computerized mapping systems to guide placement. These electrical catheters first enter the right atrium. Because atrial fibrillation begins in the left atrium a long needle will be used to cross from the right to the left side through the thin membrane that divides the 2 top chambers. This will be performed twice using both ultrasound and XRay control. This is a routine procedure called trans-septal puncture. Because the short circuits can originate from any of the pulmonary veins we will electrically isolate all 4 of these veins by performing circumferential ablation. Usually approximately 30-40 minutes of ablation is required. This part of the procedure usually takes approximately 90 minutes. The entire atrial fibrillation ablation procedure may take 3-4 hours on average. If you have persistent atrial fibrillation, additional ablation may be required.

This depends on the type of atrial fibrillation that you have.
Paroxysmal atrial fibrillation starts and stops by itself within 7 days.
The success rate for this type of atrial fibrillation is approximately 80-85%. This can vary slightly according to the type of heart problem that you have. In approximately 20-30% of patients it is necessary to perform a second procedure if the first was not successful. Even after 2 procedures, approximately 15% of patients will continue to have problems.
Persistent atrial fibrillation continues for more than 7 days or doesn’t ever stop without a DC shock (cardioversion).
The success rate for this type of atrial fibrillation is approximately 70%. This can vary slightly according to the type of heart problem that you have. In approximately 20-30% of patients it is necessary to perform a second procedure if the first was not successful. Even after 2 procedures, approximately 30% of patients will continue to have problems.
If your atrial fibrillation has been continuous for more than a year, the success rate may be lower. This will be discussed with you.
Atrial fibrillation ablation is designed to cure your symptoms and improve your quality of life. However, because the procedure carries a small risk of a major complication we recommend it only to those people having frequent episodes of atrial fibrillation or continuous atrial fibrillation where there is a significant impact on quality of life. We do not recommend the procedure for people who have minor or no symptoms or who feel that the condition represents only a relatively minor nuisance. We would also usually recommend a trial of medications first as some people will be well controlled on tablets (we understand that some people do not wish to take or cannot tolerate medications).

You will receive a letter from the hospital bookings clerk or from the Doctors secretary outlining the date of your procedure and date and time of your admission to the hospital.
In some cases a letter asking you to cease taking your medication is enclosed. This generally refers only to the medication you are taking for your abnormal heart rhythm. Your doctor will specify which medications he wants you to stop. These are usually stopped approximately 5 days prior to your procedure. If you are taking warfarin this will usually be continued but the dose may be varied in the days before the procedure based on your blood test results. If you are taking other blood thinners (Pradaxa, Xarelto or Eliquis) these would be stopped approximately 24-48 hours before the procedure and instructions will be provided.
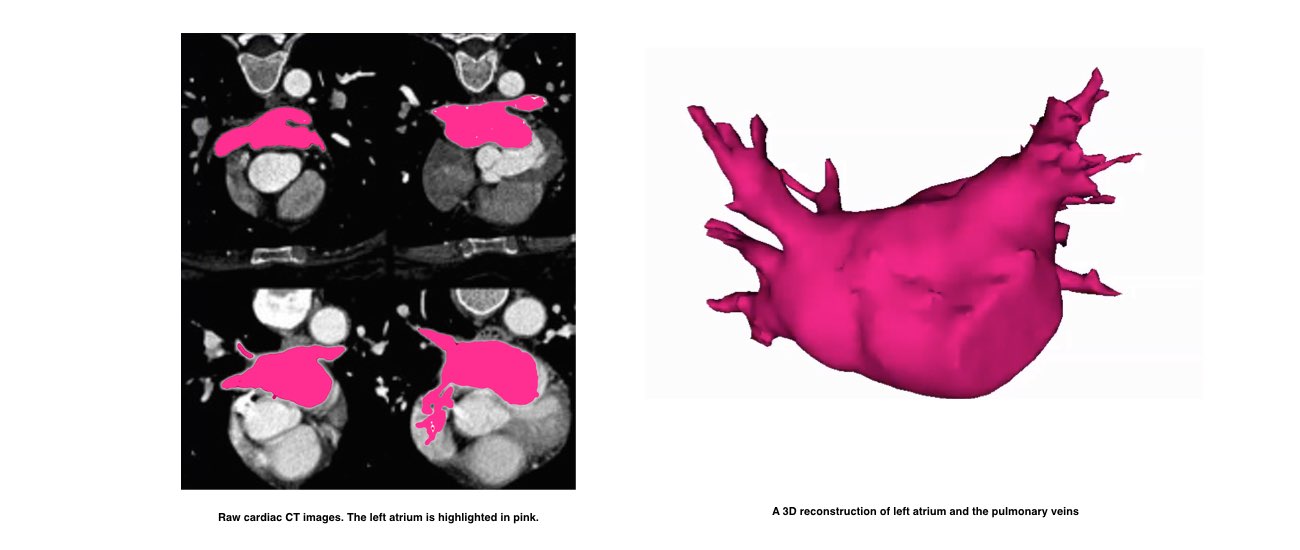
On the day before the procedure, a CT scan of your heart will be performed. This will be used during your ablation procedure.
Patients having the procedure at the Royal Melbourne Hospital will be required to attend our Pre-admission clinic on the day prior to your procedure where you will see a doctor who will record your medical history. You will also require an ECG and blood test. The doctor will also confirm the time you should be at the hospital for admission the following day.
You will be required to fast for at least six hours before the study. If your procedure is in the afternoon you may have a light early breakfast. If your procedure is in the morning, DO NOT EAT OR DRINK AFTER MIDNIGHT, except for a sip of water to help you swallow your pills.

After the procedure you will wake up in a hospital ward called the recovery area. When you are completely awake you will be transferred to the normal hospital ward. You will have to lie flat for approximately 6 hours after the procedure. During this time, it is important to keep your legs straight and your head relaxed on the pillow. You will have a compression clamp on the groin area which stays in place for 4-6 hours. You will also have a urinary catheter which will be removed later that evening or the next morning.
It is usual to stay in hospital for 2 nights after the procedure. Your heart rhythm may be monitored during this time. During this time you will either continue warfarin or commence blood thinning injections. If you are taking Pradaxa, Xarelto or Eliquis, these will be restarted on the day you go home.
It is common to have a sore throat and some mild chest discomfort after the procedure. You will also have some discomfort and bruising in the groin (and neck area in the occasional case when the neck vein is required) after the procedure. This should usually improve over several days.
Because it takes several weeks for the areas of ablation to heal and form scars, it is not uncommon to experience abnormal or irregular heart beat or rhythm for up to 4 weeks after the procedure. Rarely, atrial fibrillation may be worse for a few weeks after the procedure due to inflammation where the ablation was performed.
The majority of patients have approximately 1-2 weeks away from work.
After you go home, you will have an appointment for review with the consultant cardiologist who performed the procedure in the following 4-8 weeks.
Radiofrequency ablation for atrial fibrillation has been developed over more than 10 years and is now a routine procedure in many hospitals around the world. Approximately 10 of these procedures are performed in a usual week at the Royal Melbourne and Melbourne Private Hospitals (Over 1500 AF ablations have been performed at these hospitals -November 2013). Although most people undergoing atrial fibrillation ablation do not experience any complications, you should be aware of the following possible risks (these will be discussed with you).
The risk of any complication is approximately 4 to 6%.
The risk of a major or serious complication is approximately 1 or 2% (1 to 2 in 100).
The risk of DEATH as a complication of the procedure is approximately 1 in 1000.
Major complications (1-2% risk) include but are not limited to:
Rare but serious complications include:
Other less severe complications include: