Ventricular Tachycardia in Normal Hearts
(Idiopathic VT)
(Idiopathic VT)
Ventricular tachycardia (VT) is an abnormal rapid heart rhythm originating from the lower pumping chambers of the heart (ventricles). The normal heart usually beats between 60 and 100 times per minute, with the atria contracting first, followed by the ventricles in a synchronized fashion. In VT, the ventricles beat at a rapid rate, typically from 120 to 300 beats per minute, and are no longer coordinated with the atria.
The controlled contraction of the ventricles is important for the heart to pump blood to the brain and the rest of the body and to maintain a normal blood pressure. Abnormal and fast rhythms from the ventricle may impair the ability of the pump to supply blood to the brain and the rest of the body as a result of the rapid rate and weak contractions. This may result in palpitations (a feeling of rapid or abnormal heart beat), dizziness, lightheadedness, or syncope (loss of consciousness).
Ventricular Tachycardia (VT) occurs most commonly in patients with structural heart disease such as weakened heart muscle (cardiomyopathy) or when scar tissue develops in the heart as a result of myocardial infarction. In this situation the mechanism is usually due to re-entry circuits formed within areas of abnormal scar.
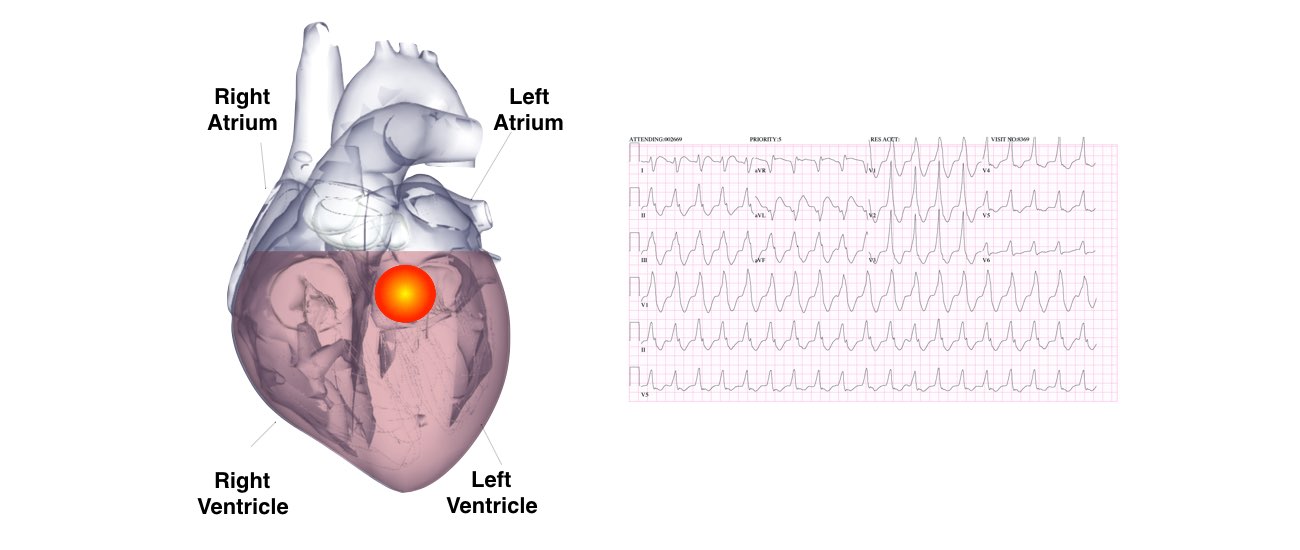
VT can also occur in patients with normal hearts, so-called “Idiopathic Ventricular Tachycardia” and this accounts for about 10% of all VTs. Idiopathic
Ventricular Tachycardia is usually due to a different mechanism than VT seen in the presence of structural heart disease. Idiopathic VT is usually due to a small nest (focus) of overly excitable heart tissue that fires of erratically, like a muscle twitch.
Overall this form of VT generally has a much better prognosis that VT in the presence of structural heart disease and is not usually associated with a risk of sudden cardiac. High-risk patients (recurrent syncope and sudden cardiac death survivors) with inherited ion channelopathies predisposing them to VT benefit from the insertion of an implantable cardioverter-defibrillator (ICD).
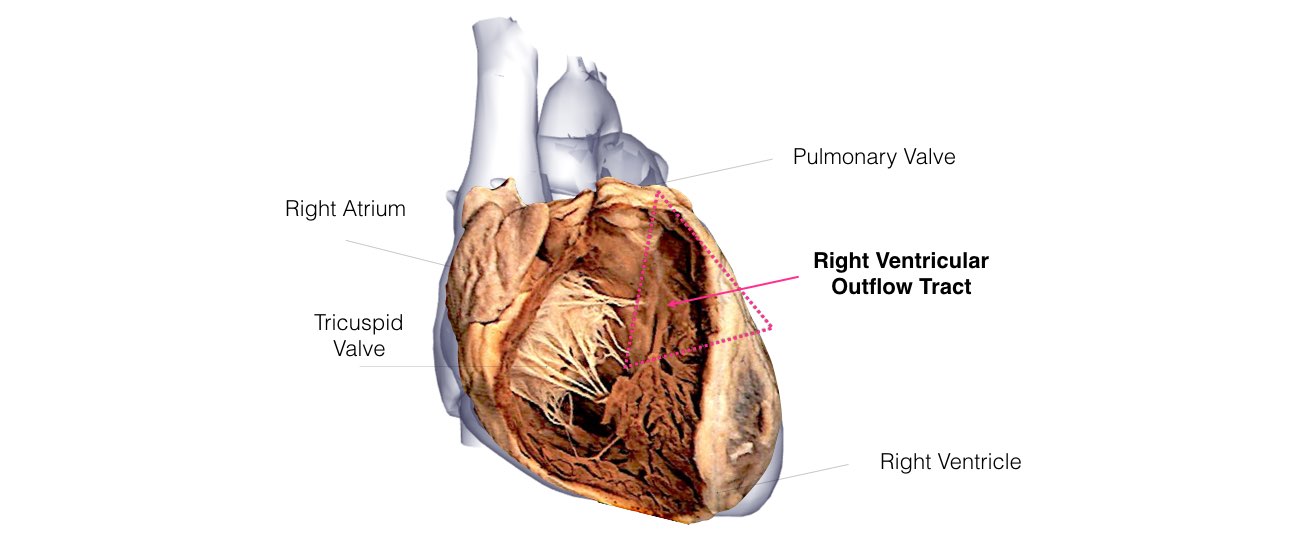
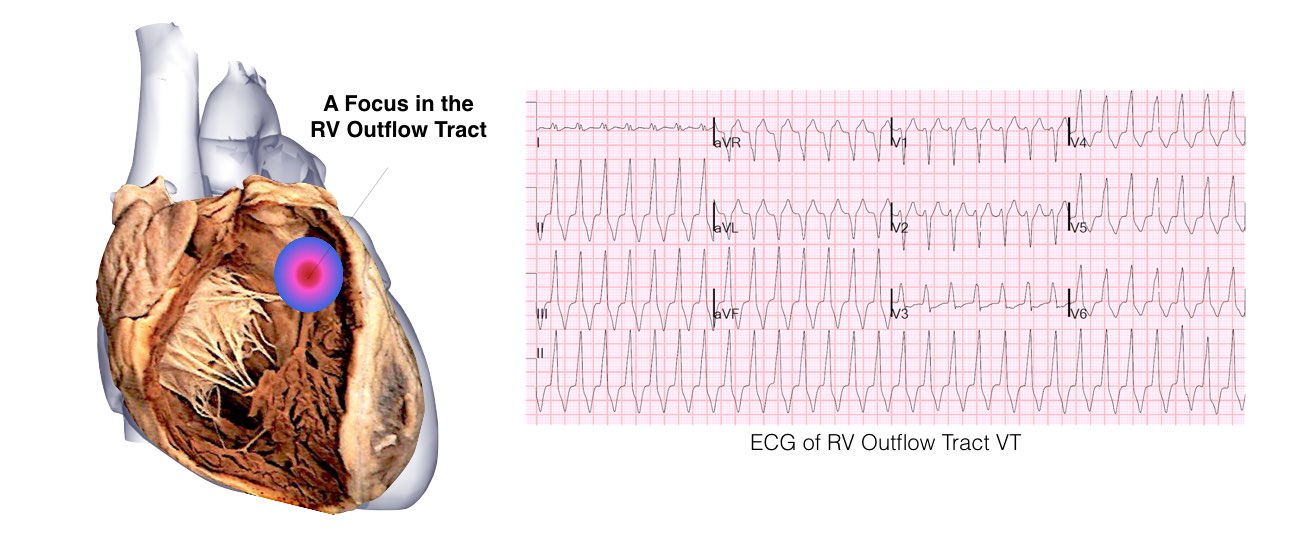
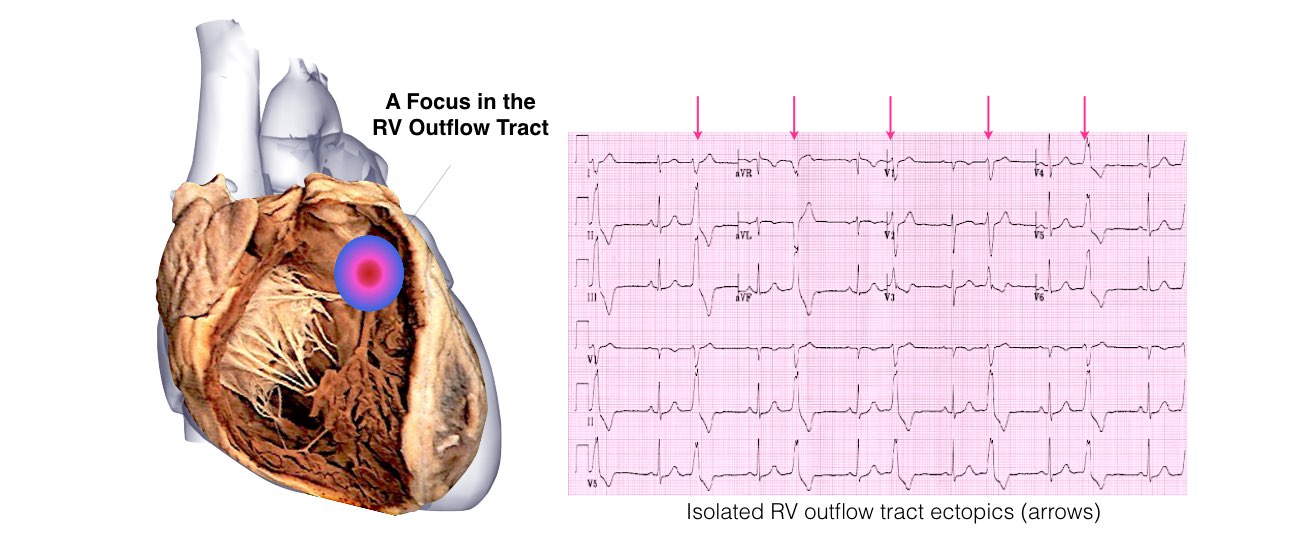
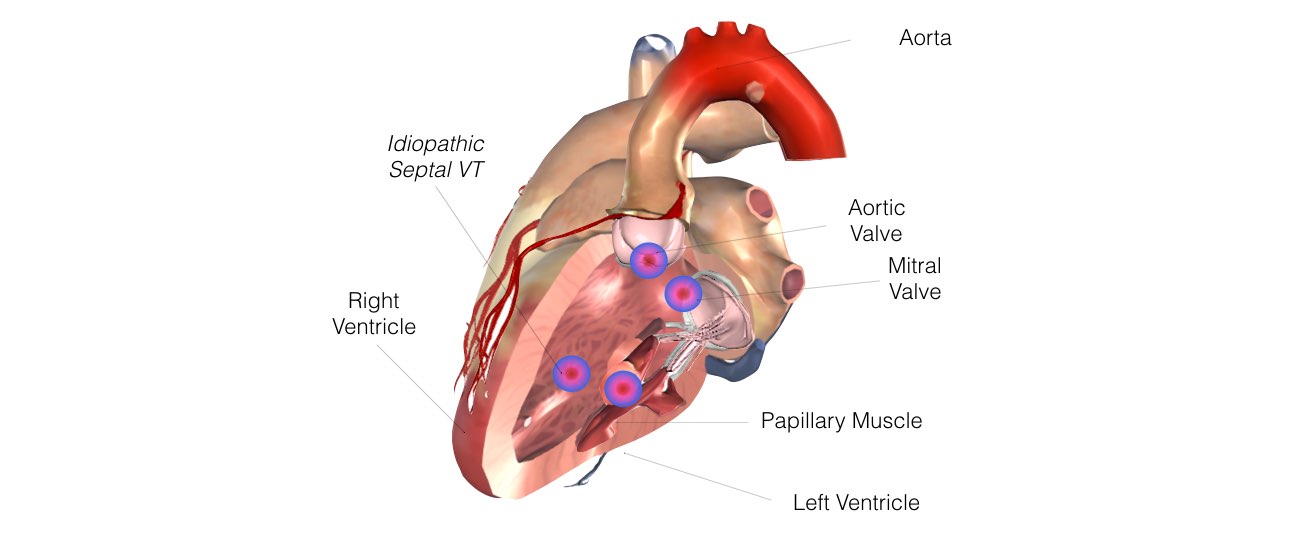
Idiopathic VTs can originate from a variety of locations such as the inside surface of the heart (endocardial), deep within the ventricular muscle (mid-myocardial), the outside surface (epicardial) of the heart, in the aortic valve or in the veins surrounding the heart. The most common form of idiopathic VT is right ventricular outflow tract VT (so (RVOT-VT). It accounts for approximately 70% of idiopathic VTs. The right ventricular outflow tract is the top portion of the right ventricle and is situated just below the pulmonary valve. This form of VT is due to an abnormal nest of cells that fires off erratically to cause either sustained VT or isolated extra beats (called ventricular ectopics). Some idiopathic VTs also form in the aortic valve (aortic cusps) or just beneath the aortic valve in the left ventricle, these are called left ventricular outflow tract VT (LVOT-VT).

There are 2 main treatment options for VT in patients without structural heart disease, medications or catheter ablation. For RVOT VT medications may be prescribed to suppress VT such as beta-blockers (Metoprolol or Atenolol) or calcium channel blockers (Verapamil or Diltiazem), however these medications only have a 25-50% rate of efficacy. Alternate therapy includes anti arrhythmic medications such as Flecainide, Sotalol and Amiodarone can also be trialed if simple beta-blockers or calcium channel blockers are ineffective. Amiodarone, the most effective drug, has many side effects, which can involve toxicity to the vital organs like the liver, thyroid, lungs, eyes, and skin.
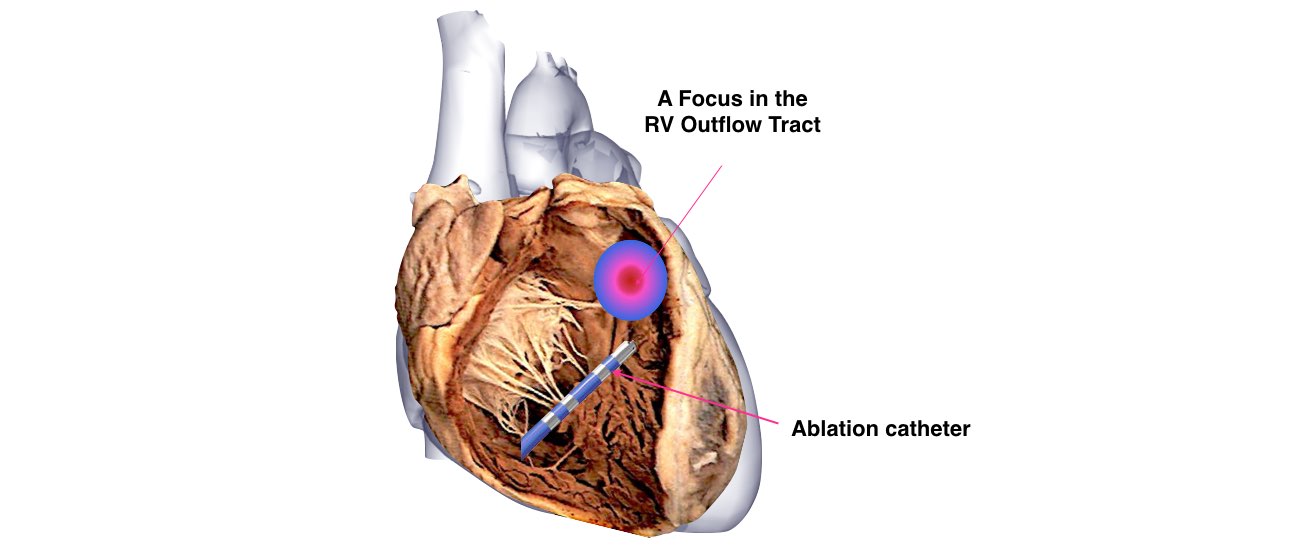
Catheter ablation of RVOT-VT now has cure rates approaching 90%, which makes it a preferable option given the young age of patients with RVOT VT. Ablation of other outflow tract sites such as the aortic cusps has also been successful. Catheter ablation is an excellent choice for patients when medications are not effective, tolerated, or preferred.
The aim of this procedure is to target the abnormal focus of the VT by placing a long, thin wire or catheter into the heart chambers through the veins of the leg. When the VT focus is identified, radiofrequency energy is applied to a small area (4 to 5 mm in diameter) to destroy the abnormal tissue. The number of burns required to treat the VT varies among patients.