BACKGROUND
The purpose of the cardioversion is to interrupt the abnormal electrical circuit(s) in the heart and to restore a normal heartbeat. The delivered electrical shock causes all the heart cells to contract simultaneously, thereby interrupting and terminating the abnormal electrical rhythm (typically fibrillation of the atria) without damaging the heart. The heart’s electrical system then restores a normal heartbeat.
The Heart
The heart is a pump responsible for maintaining blood supply to the body. It has four chambers. The two upper chambers (the right atrium and left atrium) are the chambers which receive blood as it returns from the body via the veins. The lower chambers (the right and left ventricle) are the chambers responsible for pumping the blood out to the body via the arteries. Like any pump, the heart has an electrical system that controls how it functions.
Normal heart rhythm.
In order for the heart to do its work (pumping blood throughout the body), it needs a sort of spark plug or electrical impulse to generate a heartbeat. Normally this electrical impulse begins in the upper right chamber of the heart (in the right atrium) in a place called the sino-atrial (SA) node. The SA node is the natural pacemaker of the heart. The SA node gives off electrical impulses to generate a heartbeat in the range of 60 to 100 times per minute. If you are exercising, doing strenuous work or you are under a lot of stress, your heart rate may be faster. When you rest or sleep your heart rate will slow down. If you take certain medications, your heart rate may be slower.
From the SA node, the electrical impulse is relayed along the heart’s conduction system. It spreads throughout both the right and left atria causing them to contract evenly. When the impulse spreads over the right atrium it reaches the atrio-ventricular (AV) node. This is a very important structure in the heart because it is the only electrical connection between the top chambers and the bottom chambers. It is therefore the only way in which an electrical impulse can reach the pumping chambers (the ventricles). The impulse spreads through the AV node and down into the lower chambers or ventricles of the heart. This causes them to contract and pump blood to the lungs and body.
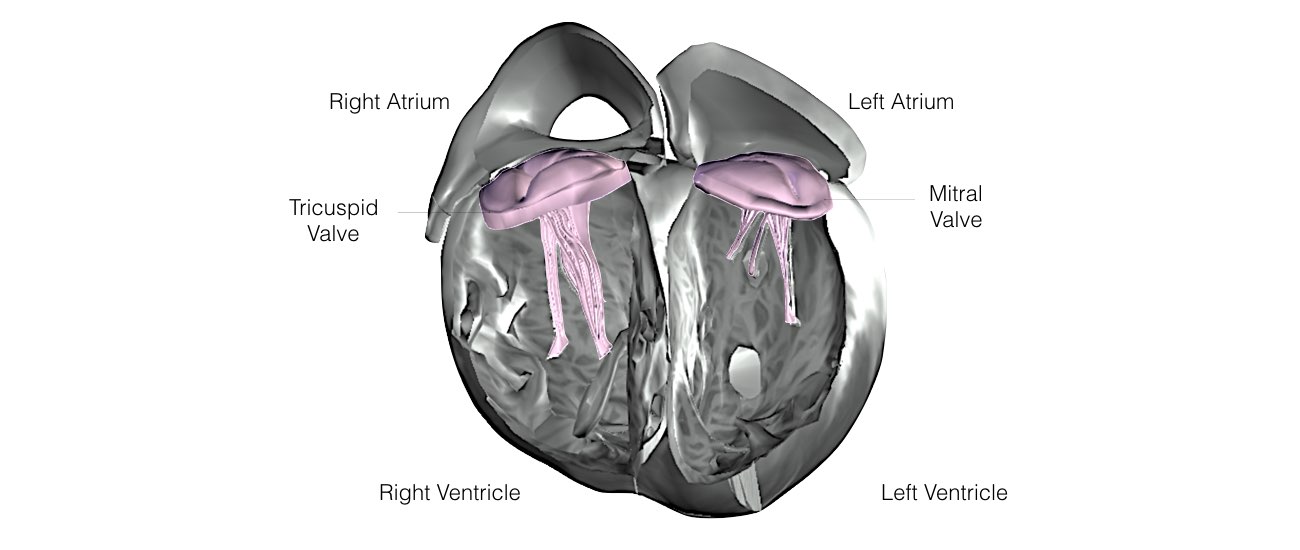
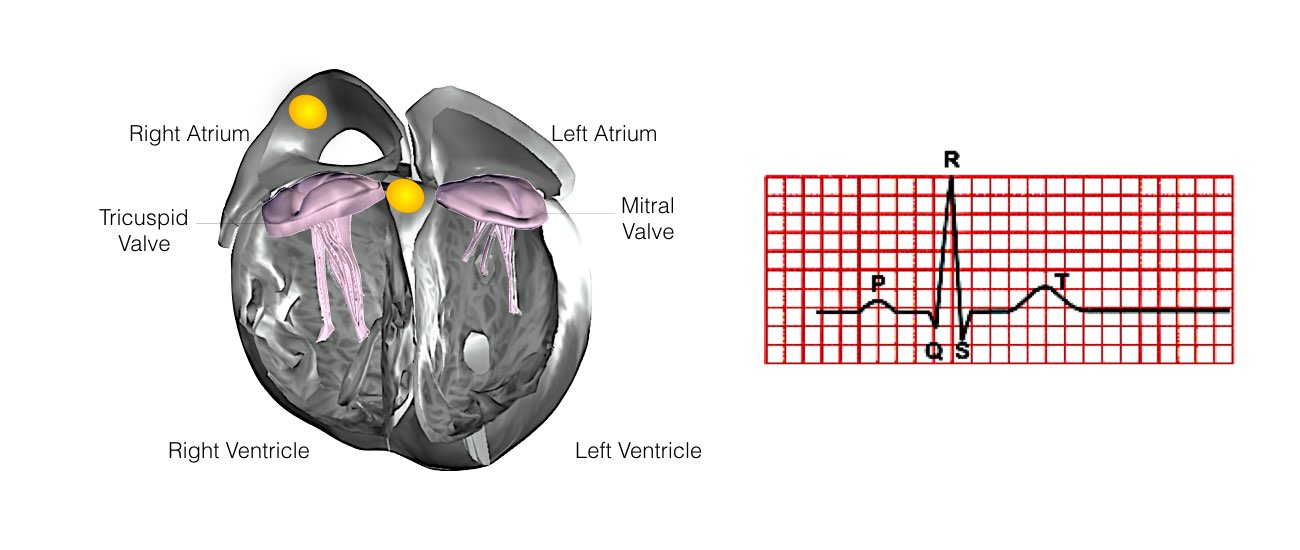
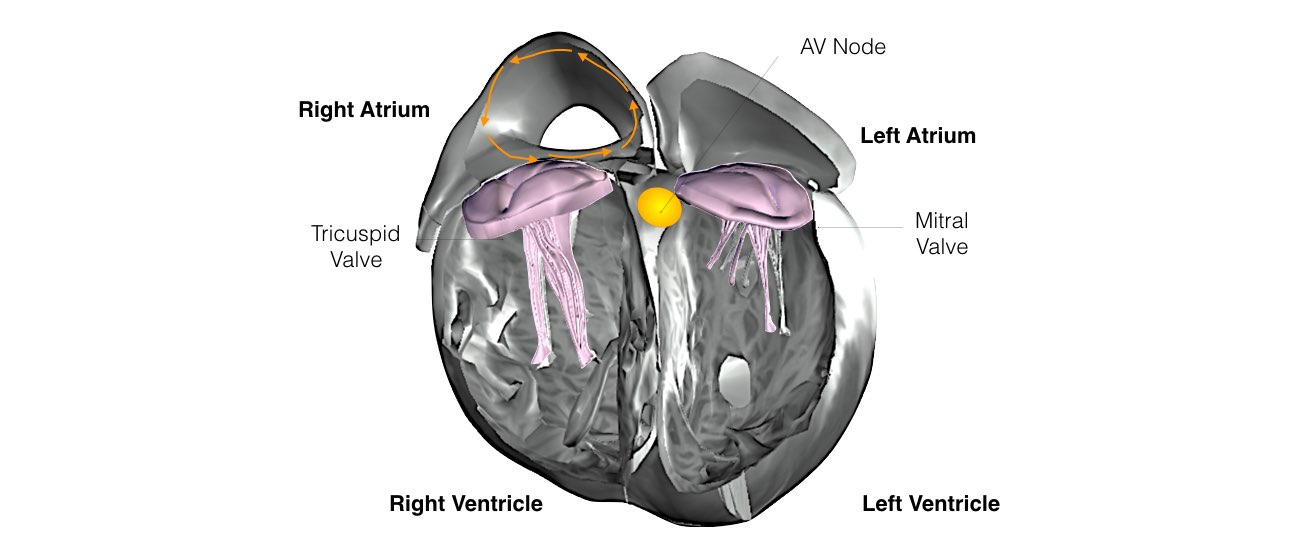
The heart is made up of four chambers. The top two chambers are call the Atria and the bottom two chambers are called the Ventricles.
The top and bottom chambers are separated by two valves the Tricuspid Valve and the Mitral Valve.
The Tricuspid Valve separates the Right Atrium from the Right Ventricle
The Mitral Valve separates the Left Atrium from the Left Ventricle
Slide 1 of 8
The top and bottom chambers are separated by two valves the Tricuspid Valve and the Mitral Valve.
The Tricuspid Valve separates the Right Atrium from the Right Ventricle
The Mitral Valve separates the Left Atrium from the Left Ventricle
Slide 1 of 8
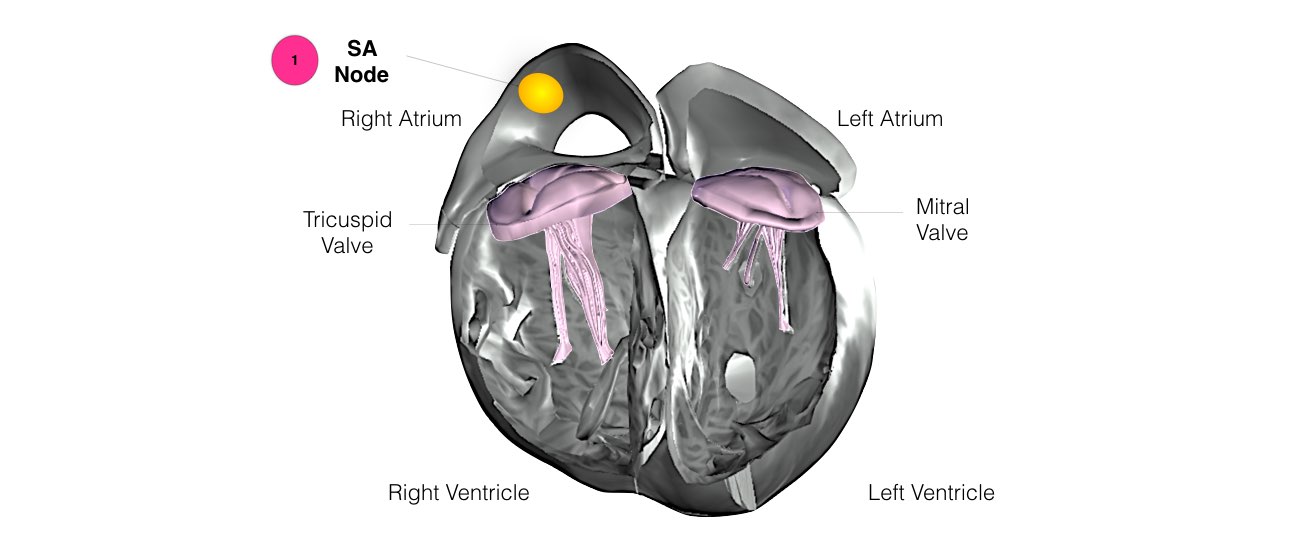
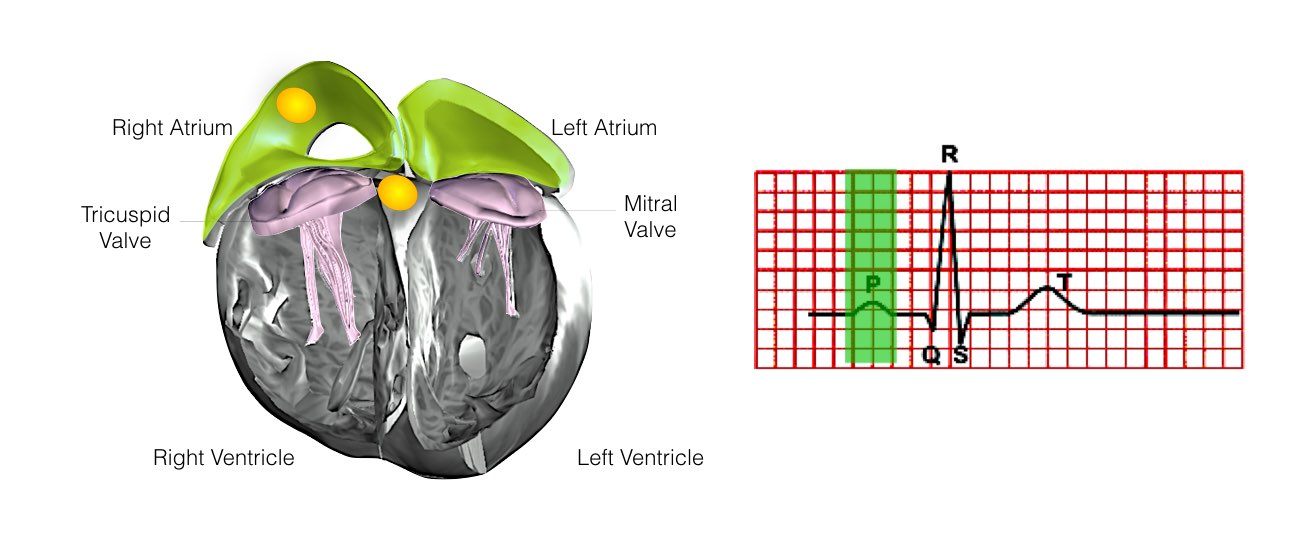
1) The normal heart beats starts in the Sino-Atrial Node located in the Right Atrium. This acts as the spark plug to start the heart.
Slide 2 of 8
Slide 2 of 8
The normal heart beats starts in the Sino-Atrial Node located in the Right Atrium. This acts as the spark plug to start the heart.
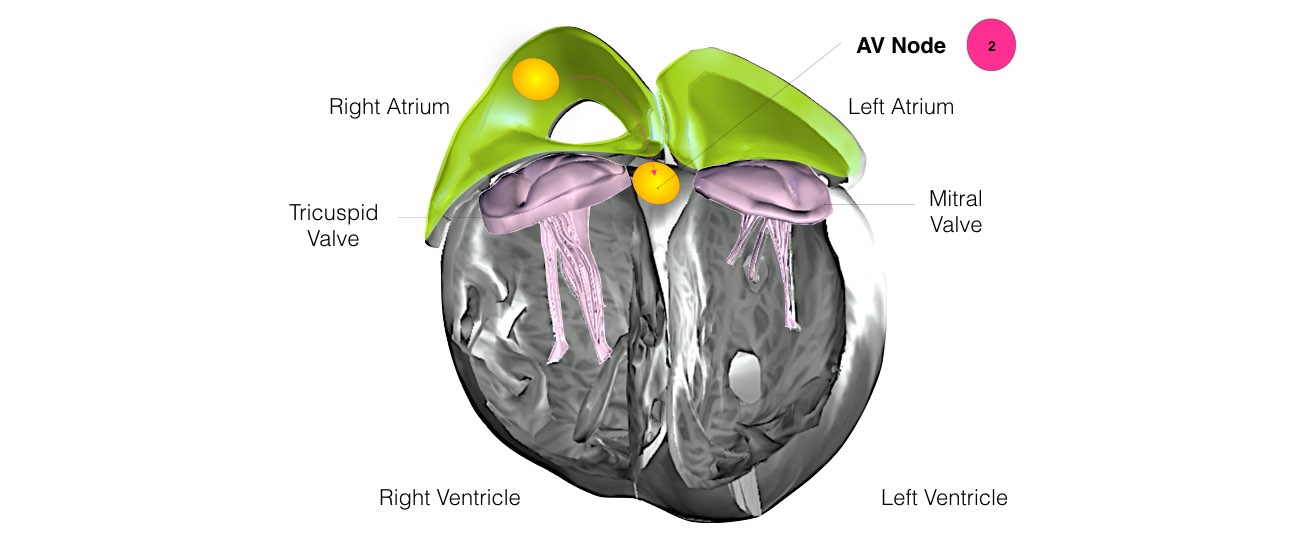
2) Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
Slide 3 of 8
2) Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
Slide 3 of 8
The normal heart beats starts in the Sinus Node located in the Right Atrium. This acts as the spark plug to start the heart.
Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
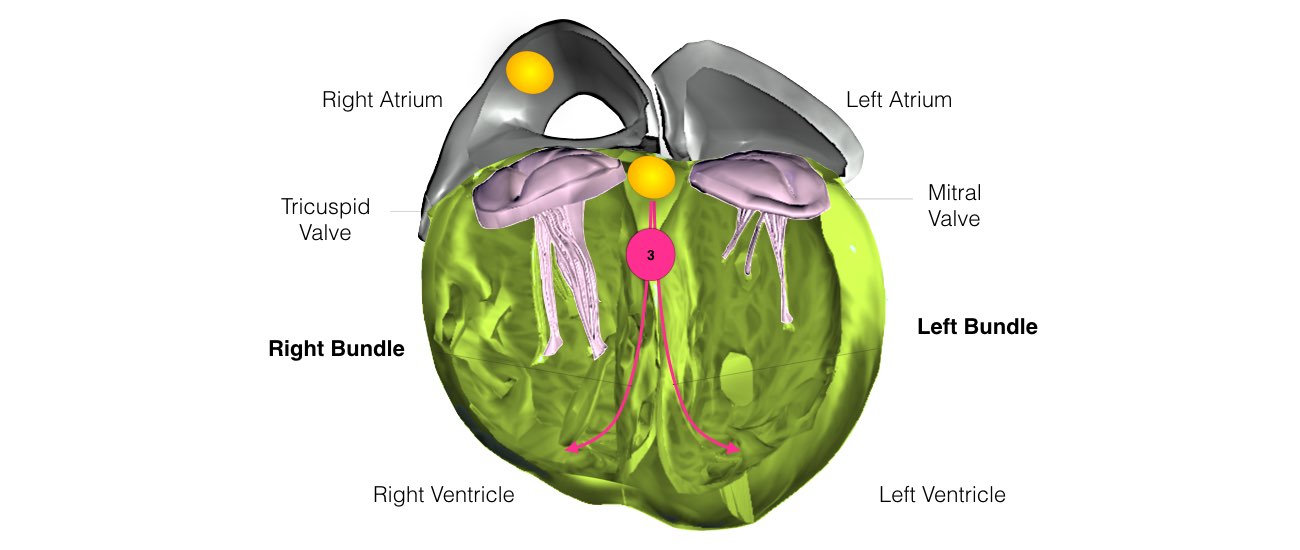
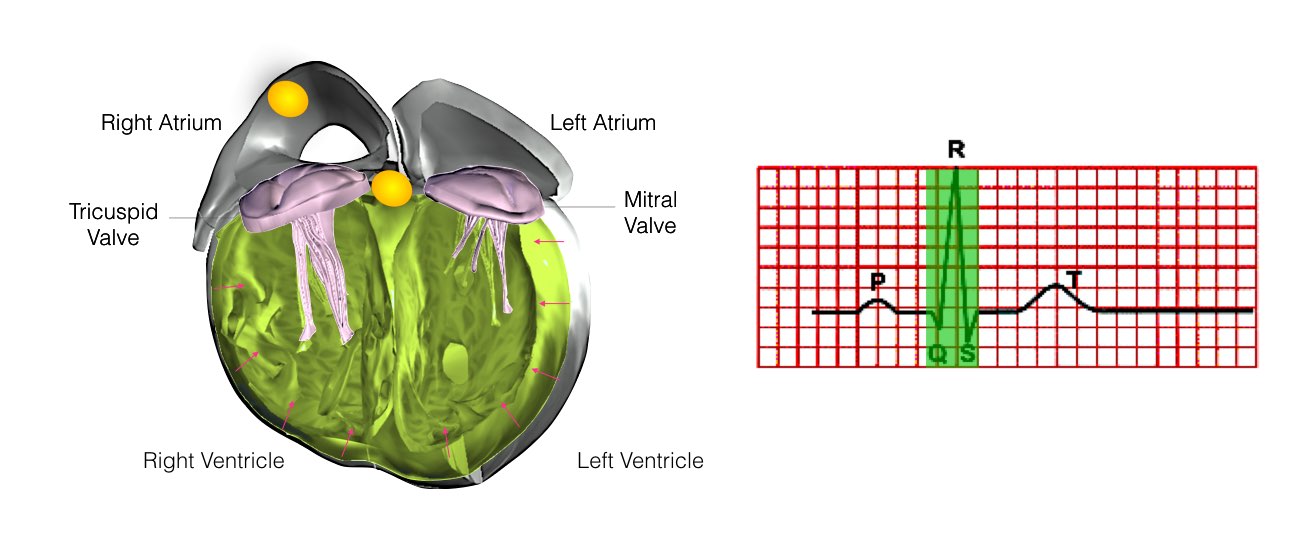
3) After electrical conduction passes through the AV node it travels down the Left and Right Bundle Branches which activates the Ventricles and tells them to contract.
Slide 4 of 8
Electrical conduction then activates both atria and travels to a structure called the AV-Node. The AV node acts as the ‘gate keeper’ of all electrical impulses to the ventricles.
3) After electrical conduction passes through the AV node it travels down the Left and Right Bundle Branches which activates the Ventricles and tells them to contract.
Slide 4 of 8
The heart's normal contraction can be seen on the ECG. This ECG shows normal sinus rhythm and is made up of a series of waves called the P, QRS and T wave.
Slide 5 of 8
Slide 5 of 8
Atrial activation is represented by the ‘P-Wave’ on the ECG.
Slide 6 of 8
Slide 6 of 8
Ventricular activation is represented by the ‘QRS’ complex on the ECG. This normally takes less than 120 milliseconds.
During this time the Ventricles contract and blood is pumped from the heart to the lungs and through the aorta to the rest of the body.
Slide 7 of 8
During this time the Ventricles contract and blood is pumped from the heart to the lungs and through the aorta to the rest of the body.
Slide 7 of 8
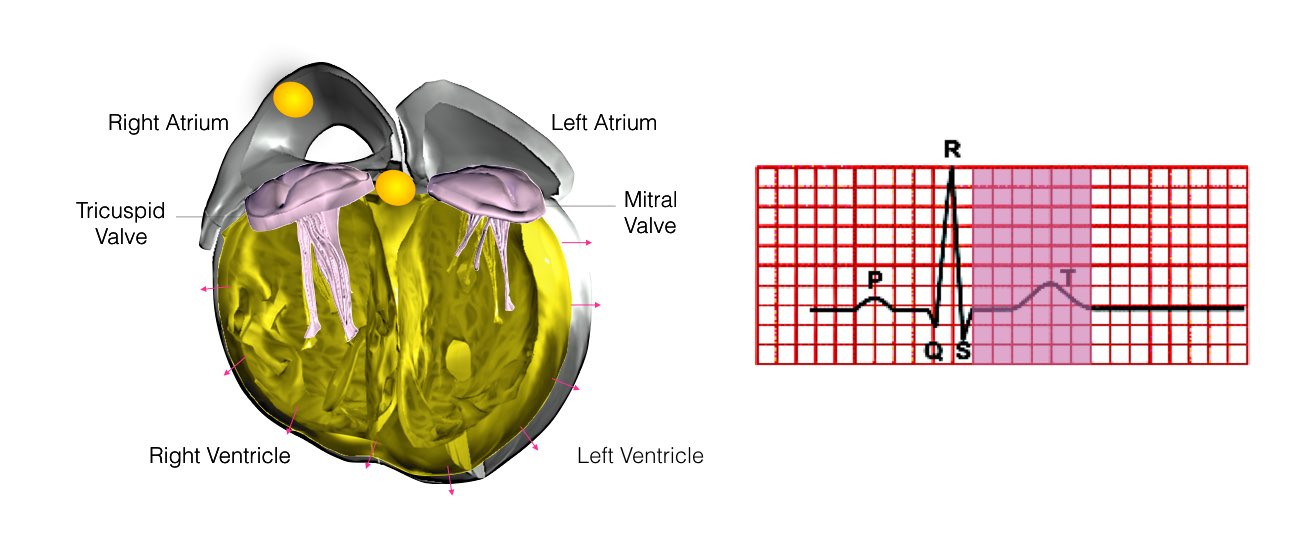
The final wave is called the T wave. During this phase the Ventricles relax. This normally takes less than 450 milliseconds.
Slide 8 of 8
Slide 8 of 8
Who requires EPS?
Patients are referred for EPS for many reasons.
Some of the more common reasons are:
- rapid or irregular heart beat (often associated with shortness of breath, chest pain or dizziness). Common terms used are palpitations, racing heart or missed beats.
- blackout or dizziness.
- abnormal findings on an ECG.
How do abnormal heart rhythms occur?
In some hearts, an abnormal heart rhythm develops when an electrical impulse either starts from a different location, other than the SA node, or follows a route (or pathway) that is not normally present.
Your doctor will explain the exact nature of your abnormal heart rhythm and the following diagrams should help you understand the mechanism.
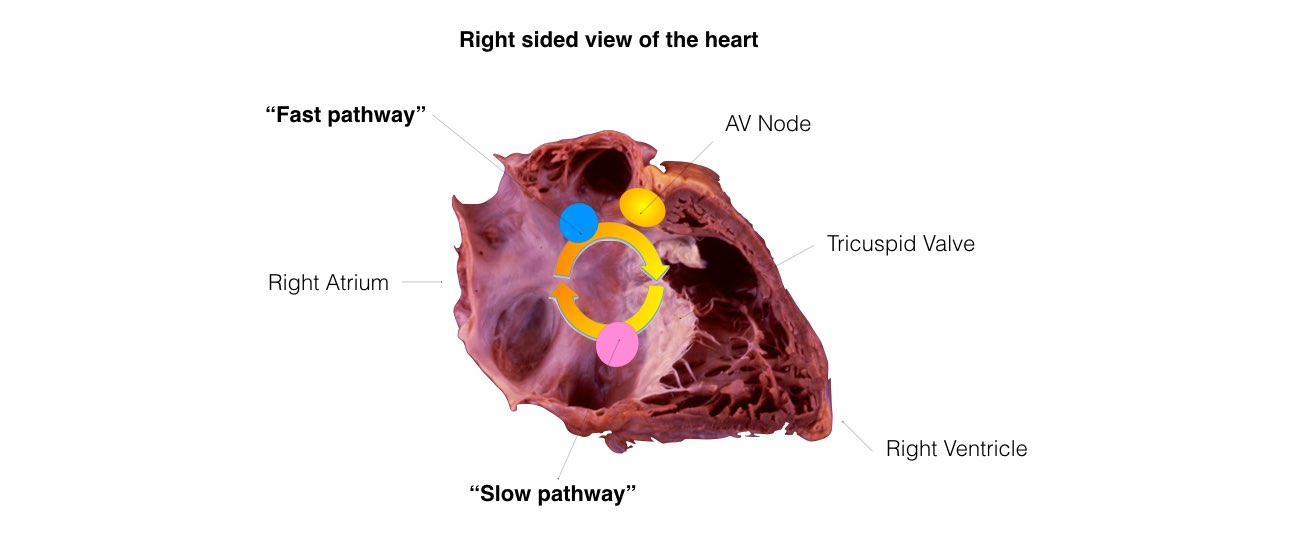
In AV Nodal Re-entry Tachycardia a ‘short-circuit’ is formed between two normal conducting fibres in the heart, called the “fast pathway” (blue) and
the “slow pathway” (pink).
This simple re-entry circuit is one of the most common causes of supra ventricular tachycardia. This ‘short-circuit’ can be treated with a simple procedure called radio-frequency ablation.
Slide 1 of 7
This simple re-entry circuit is one of the most common causes of supra ventricular tachycardia. This ‘short-circuit’ can be treated with a simple procedure called radio-frequency ablation.
Slide 1 of 7
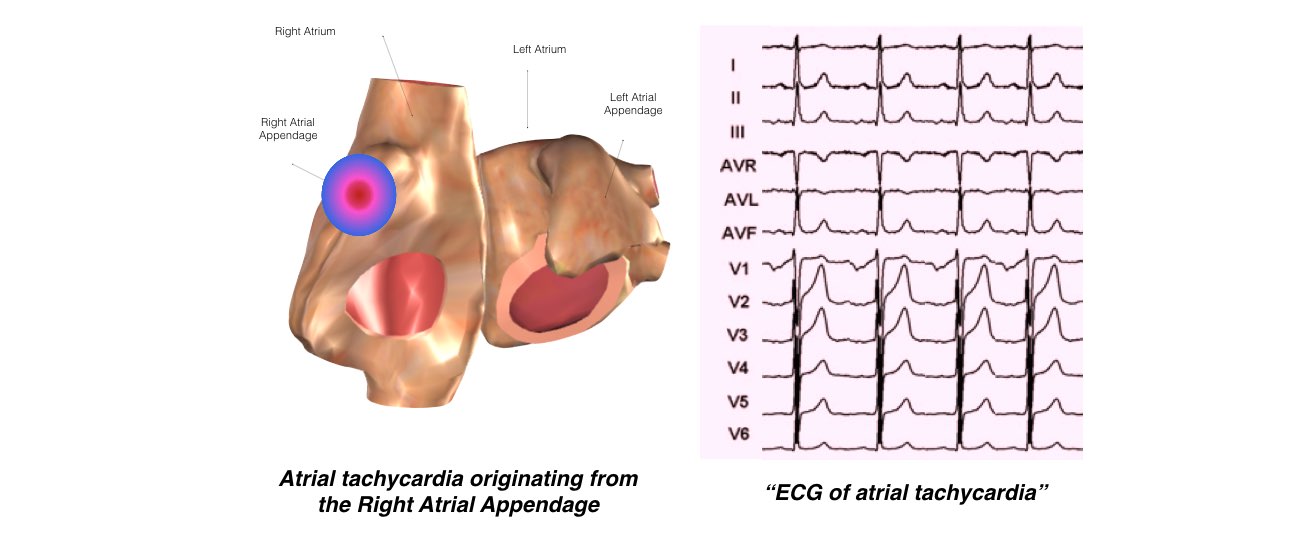
Atrial tachycardias are caused by small nests of rapidly firing cells within normal atrial tissue. They are called focal tachycardias.
Rapid firing of these abnormal cells leads to a rapid heart rate which can cause symptoms such as palpitations and shortness of breath.
Slide 2 of 7
Rapid firing of these abnormal cells leads to a rapid heart rate which can cause symptoms such as palpitations and shortness of breath.
Slide 2 of 7
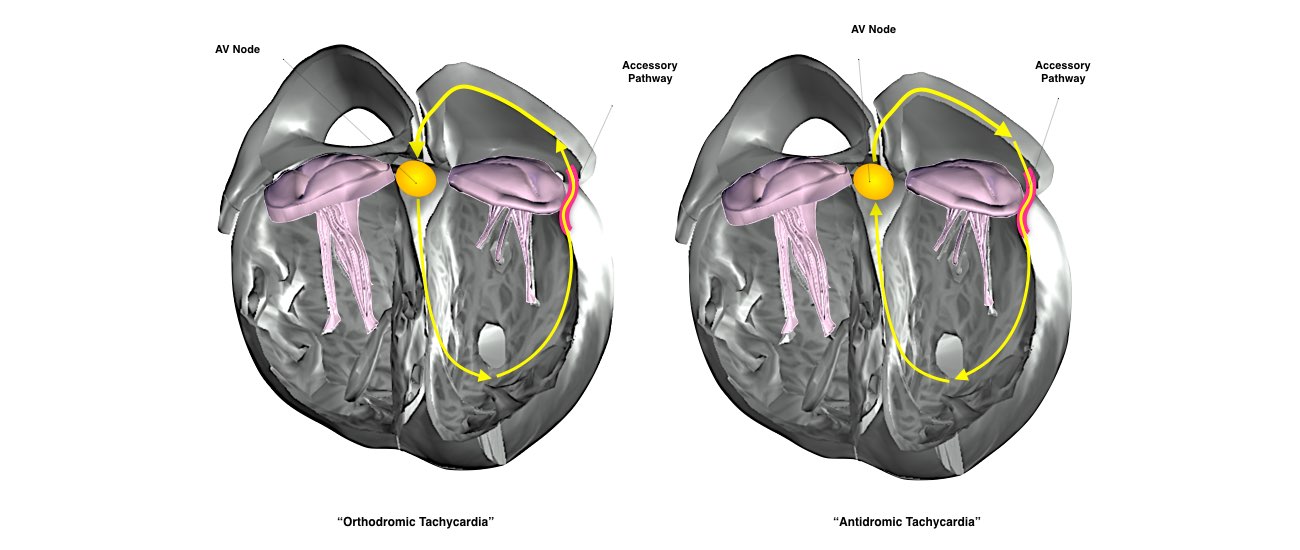
Accessory pathways provide the ‘short-circuit’ required for re-entry circuits and can result in palpitations. The two circuits that can occur are shown. The most common circuit utilises the accessory pathway to conduct from the Ventricle back to the Atrium. This is called “Orthodromic tachycardia” and leads to a narrow complex SVT on the 12 lead ECG. The other circuit uses the accessory pathway to conduct from the Atria to the Ventricles and is called “Antidromic Tachycardia”.
Slide 3 of 7
Slide 3 of 7
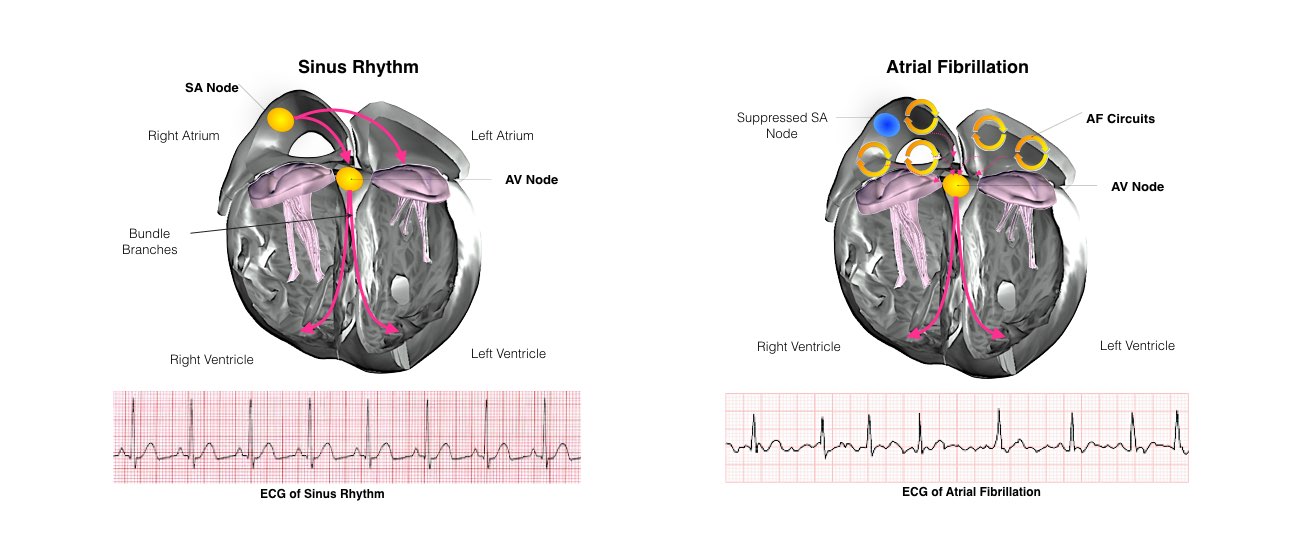
Diagram and ECG chart of Sinus Rhythm and Atrial Fibrillation for comparison.
Slide 4 of 7
Slide 4 of 7
Typical flutter is an abnormal rhythm of the right atrium.
It is a simple circuit that rotates around the right atrium at over 300 beats per minute.
The typical atrial flutter circuit is shown by the orange arrows.
Slide 5 of 7
It is a simple circuit that rotates around the right atrium at over 300 beats per minute.
The typical atrial flutter circuit is shown by the orange arrows.
Slide 5 of 7
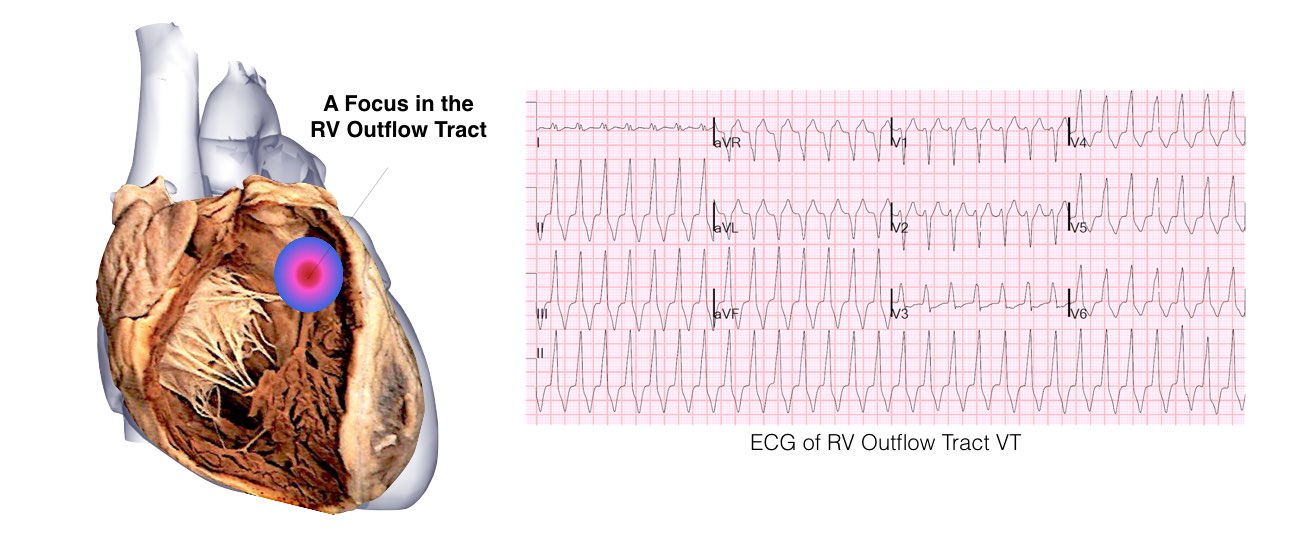
A focus of abnormal excitable tissue fires off quickly resulting in a sustained Ventricular Tachycardia.
Slide 6 of 7
Slide 6 of 7
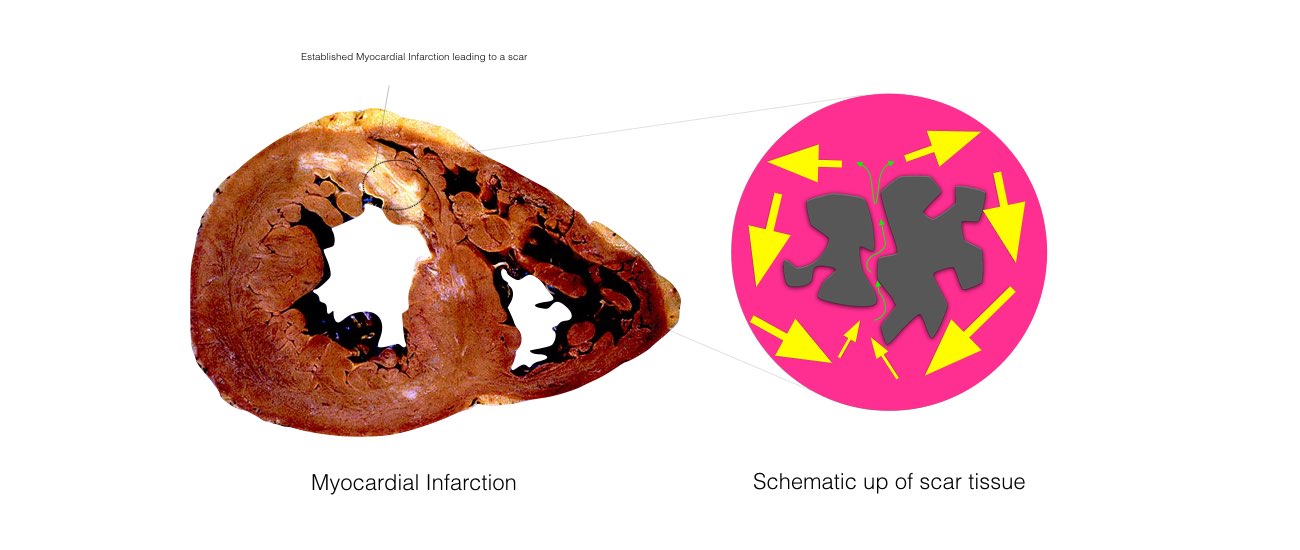
The scar can be quite large and can be of variable thickness.
The scar tissue is made up of a complex mix of areas of dead or scarred tissue (grey) and some surviving tissue(pink).
It is the complex mix of islands of scar tissue and surviving tissue that forms VT circuits.
Slide 7 of 7
The scar tissue is made up of a complex mix of areas of dead or scarred tissue (grey) and some surviving tissue(pink).
It is the complex mix of islands of scar tissue and surviving tissue that forms VT circuits.
Slide 7 of 7
