AV Node Ablation
AV node ablation and pacemaker implantation is usually reserved for patients in whom all other treatments of atrial fibrillation have been ineffective.
AV node ablation and pacemaker implantation is usually reserved for patients in whom all other treatments of atrial fibrillation have been ineffective.
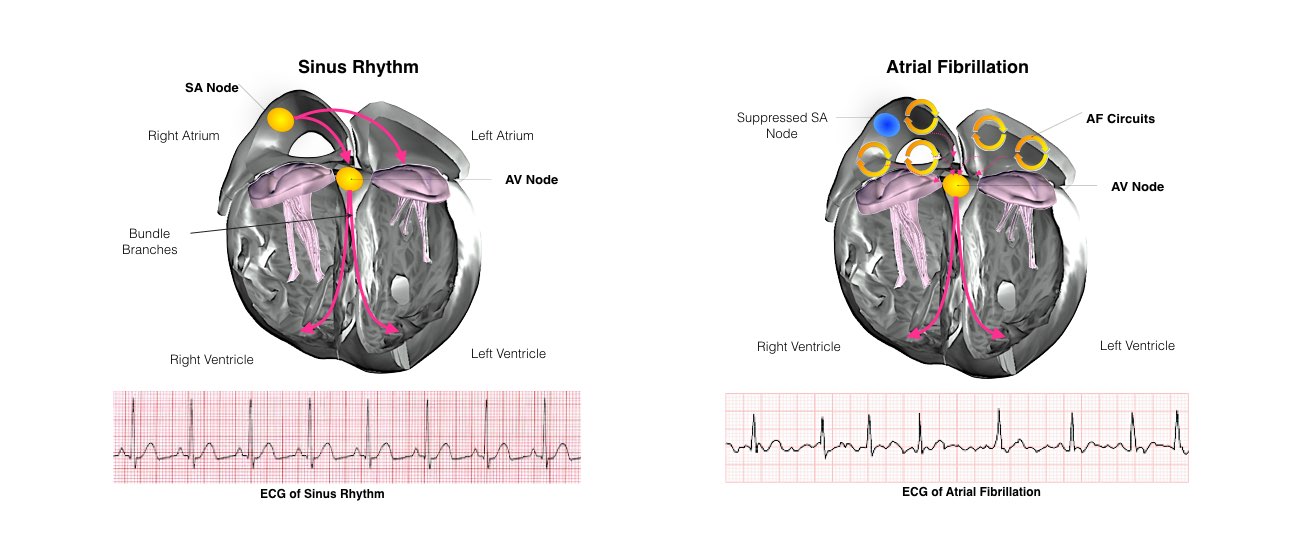
The heart is a pump responsible for maintaining blood supply to the body. It has four chambers. The two upper chambers (the right atrium and left atrium) are the chambers that receive blood as it returns from the body via the veins. The lower chambers (the right and left ventricle) are the chambers responsible for pumping the blood out to the body via the arteries. Like any pump, the heart has an electrical system that controls how it functions.
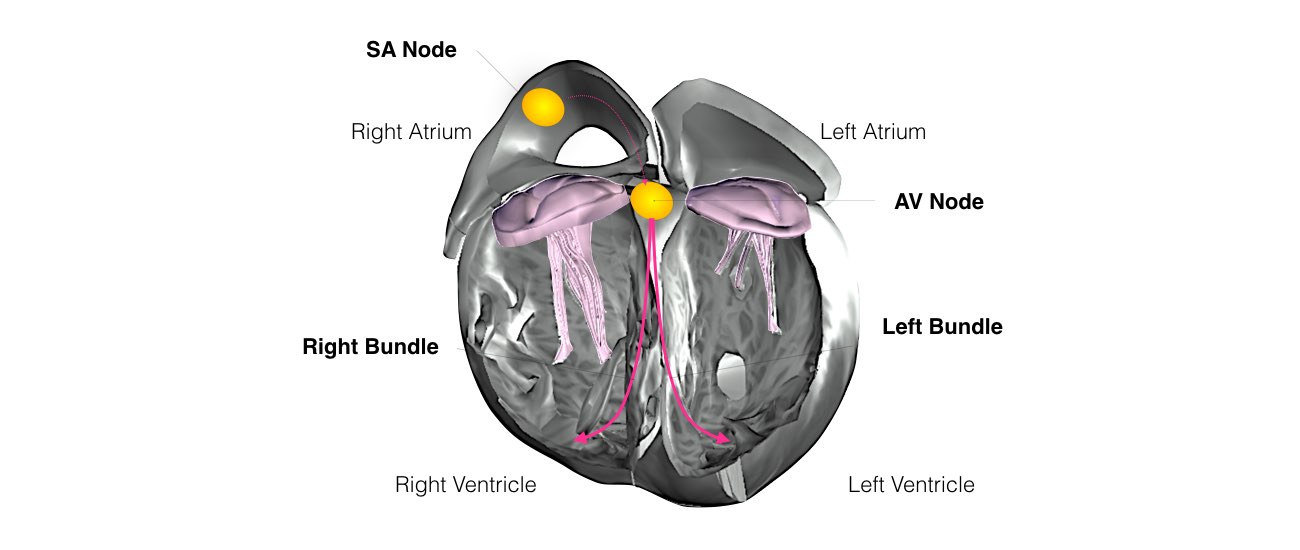
In order for the heart to do its work (pumping blood throughout the body), it needs a sort of spark plug or electrical impulse to generate a heartbeat. Normally this electrical impulse begins in the upper right chamber of the heart (in the right atrium) in a place called the sino-atrial (SA) node. The SA node is the natural pacemaker of the heart. The SA node gives off electrical impulses to generate a heartbeat in the range of 60 to 100 times per minute. If you are exercising, doing strenuous work or you are under a lot of stress, your heart rate may be faster. When you rest or sleep your heart rate will slow down. If you take certain medications, your heart rate may be slower. All of this is appropriate.
From the SA node, the electrical impulse is relayed along the heart’s conduction system. It spreads throughout both the right and left atria causing them to contract evenly.
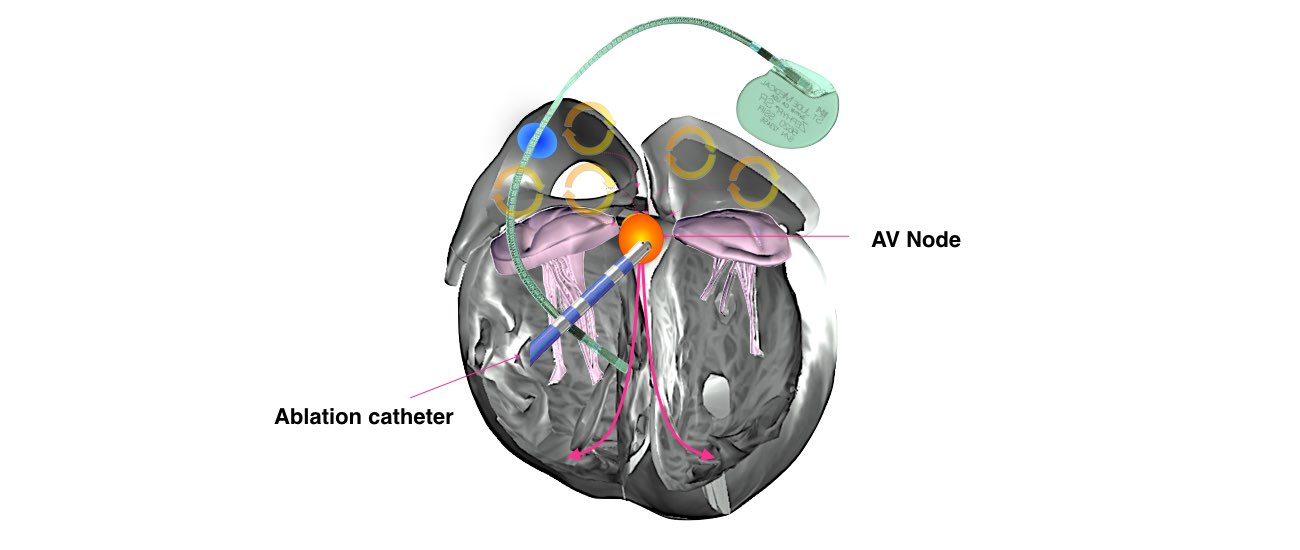
When the impulse spreads over the right atrium it reaches the atrio-ventricular (AV) node. This is a very important structure in the heart because it is the only electrical connection between the top chambers and the bottom chambers. It is therefore the only way in which an electrical impulse can reach the pumping chambers (the ventricles). The impulse spreads through the AV node and down into the lower chambers or ventricles of the heart. This causes them to contract and pump blood to the lungs and body.
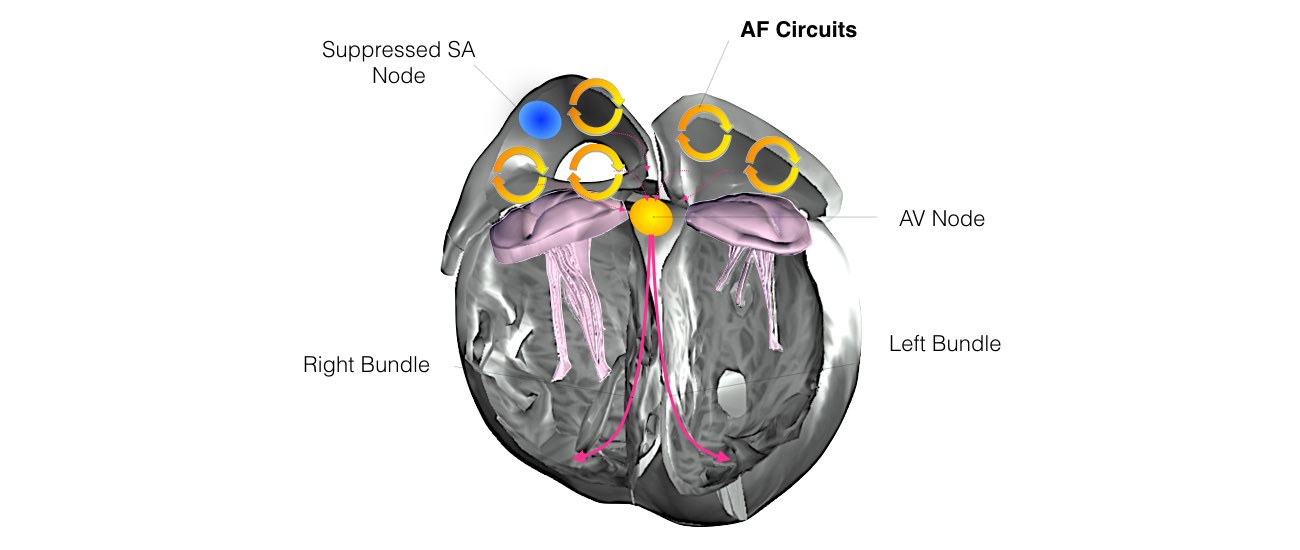
In some hearts, an abnormal heart rhythm develops when an electrical impulse either starts from a different location, other than the SA node, or follows a route (or pathway) that is not normally present. This is what happens in atrial fibrillation. Multiple electrical short circuits develop in the upper heart chambers as shown in the diagram below.
Atrial Fibrillation is due to multiple short circuits in the upper chambers of your heart termed the left and right atria. These rapid short circuits have several consequences:
AV node ablation and pacemaker implantation is usually reserved for patients who are fed up with the symptoms of atrial fibrillation which are significantly interfering with their quality of life and their lifestyle and for whom all of the medications are not effective. If you are in this category it is highly likely that you will feel very much better if you have the procedure.
AV node ablation and pacemaker implantation is usually reserved for patients in whom all other treatments of atrial fibrillation have been ineffective.
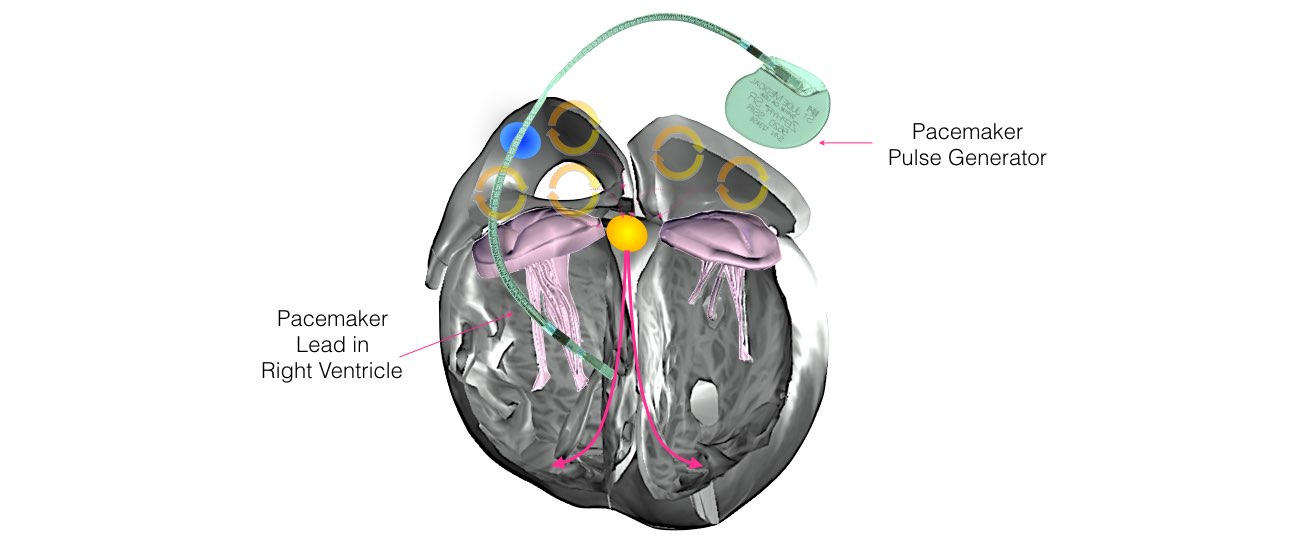
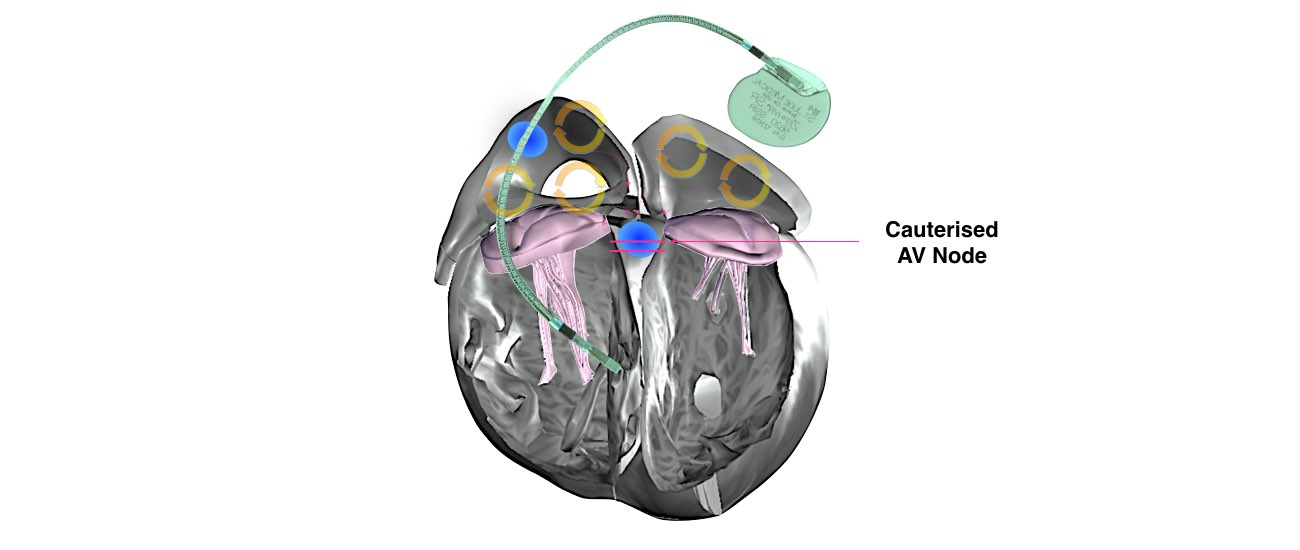
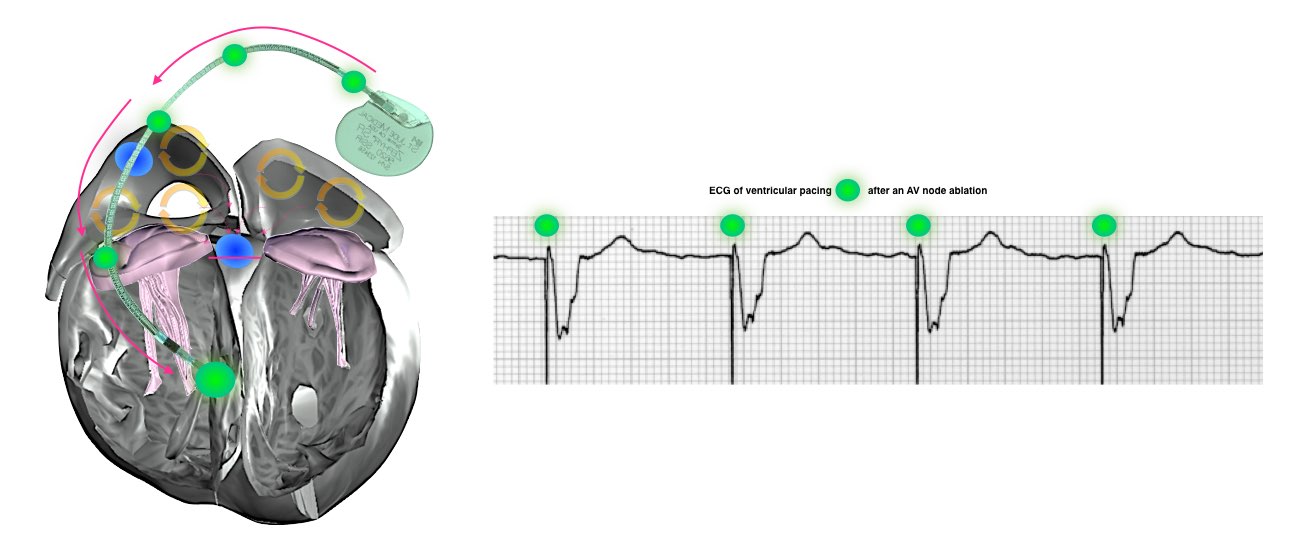
The first step is to implant the pacemaker. By itself the pacemaker will not improve the way you feel. However, following this a special procedure called AV Node ablation (sometimes also called His bundle ablation) will be performed. This procedure is a simple procedure which effectively “knocks out” the AV node. This will prevent any of the electrical short-circuits in the atria from reaching the ventricles. The pacemaker will now have complete control of your heart rhythm. The heart rhythm will be regular and will no longer race rapidly.
What is involved in Pacemaker Implantation?
Insertion of a pacemaker is a very common procedure. This is performed under local anaesthetic with sedative medication to make you feel comfortable. The procedure takes approximately 1 hour and is performed in the cardiac catheter laboratory.
This is a special room that has a patient table, X-Ray tube, ECG monitors and other equipment. The staff in the lab will all be dressed in hospital theatre clothes and during the procedure will be wearing hats and masks.
Many ECG monitoring electrodes will be attached to your chest area. A nurse or doctor will insert an intravenous line usually into the back of your hand. This is needed as a reliable way to give you medications during the procedure without further injections. You will also have a blood-pressure cuff attached to your arm that will automatically inflate at various times throughout the procedure.
The pacemaker is inserted just under the collar-bone usually on the right side. The area is prepared with a special sterile solution that may feel cold. You will be covered by a large sterile sheet that will partly cover your face. You will be able to look out from under the sheet to the side and a nurse will be present at all times. You will be given oxygen to breathe by a small tube that is positioned under your nostrils.
At the start of the procedure, the doctor will inject local anaesthetic into the area under the collar-bone where the pacemaker is to be inserted. This will sting momentarily but the area will then be numb. During the procedure you may feel some firm pushing in the shoulder area but this should not be painful. If you experience pain or discomfort you should tell the nurse or doctor.
After the procedure you will have some bruising and discomfort in the area of the pacemaker that may persist for several weeks. You should avoid strenuous activities with your arm for a period of 4 weeks. You should refrain from driving for 2 weeks.
You will be allowed to go home 1 or 2 days after the procedure.
The oxygen level of your blood will also be measured during the procedure and a small plastic device will be fitted on your finger for this purpose. Your groin will be washed with an antiseptic cleansing liquid and you will be covered with a sterile sheet.
The doctor will inject local anaesthetic to the groin area and this will sting momentarily. After that, you may feel pressure as the doctor inserts the catheters but you should not experience any pain. The doctor will then insert a special catheter through the vein in your groin area. As this is all internal you will not feel any discomfort. This will pass via your veins up into your heart. The doctor controls its position with the aid of x-ray. A small burn will be delivered to the AV node through the tip of the catheter. This essentially destroys this electrical conducting pathway.
The entire procedure takes approximately 30 minutes.
You will have to lie flat for 4 hours after the procedure.
You may have some bruising and discomfort in the groin area and you should avoid strenuous physical activity for at least 1 week.
You will be able to go home the day after the procedure.
You will receive a letter from the hospital bookings clerk or from the Doctors secretary outlining the date of your procedure and date and time of your admission to the hospital.
If you are taking anti-coagulation (blood thinning) medication eg warfarin then you will need to stop this for approximately 5 days prior to your procedure. Your doctor may arrange for you to have daily heparin injections after you stop the warfarin.
Patients having the procedure at the Royal Melbourne Hospital will be required to attend the pre-admission clinic on the day prior to the procedure.
Some country patients may need to make arrangements to stay overnight with family or friends.
At the pre-admission clinic you will see a doctor who will record your medical history. You will also require an ECG and blood test. The doctor will also confirm the time you should be at the hospital for admission the following day.
You will be required to fast for at least six hours before each of the procedures. If your procedure is in the afternoon you may have a light breakfast. If your procedure is in the morning, DO NOT EAT OR DRINK AFTER MIDNIGHT, except for sips of water to help you swallow your pills.

Pacemaker implantation is a very common and low risk procedure and should a complication arise, it will be dealt with at once.
Although most people undergoing pacemaker implantation do not experience any complications, you should be aware of the following risks:
AV Node ablation is also a very common and very low risk procedure.
Prior to both procedures, if you are taking warfarin, this will need to be stopped for several days (your doctor will advise you exactly). During the time that you are not taking warfarin, there will be a very small chance of a blood clot forming.